RESEARCH ARTICLES
Nurses' organizational commitment and relationship with supervisor
Maria Manuela Frederico FerreiraI; Isilda Cristina Laranjeira da SilvaII
IPhD in Management Sciences. Coordinating Professor, Nursing School of Coimbra. President of the Council for Quality and Evaluation. Researcher and coordinator of the line Health Systems and Organizations in Health Sciences Research Unit. Nursing. Coimbra, Portugal. E-mail: mfrederico@esenfc.pt
IIMaster in Management and health economics. Nurse in Hospital de Abrantes. Abrantes, Portugal. E-mail: isilda.cls@gmail.com
INTRODUTION
In contexts of transformation that are occurring, especially in the most developed countries, the health sector is one of the most exposed. Like in other contexts, it is unquestionable, in this sector that the success of transformations depends on the people’s involvement.
Nurses are not an exception and represent, in terms of quantity, a quite significant part of human resources allocated in health institutions and mainly in hospital institutions. By the other hand, nursing services suffer an impact of imposed policies by determining positive and negative consequences to the sector1, where it is important to know both its level of organizational commitment and the responsible factors for its promotion. Thus the study of the way how health professionals, particularly nurses, are committed to the organization where they work is increasingly more important, being accepted that commitment favours positive and productivity behaviours, among others2.
We can generically consider organizational commitment like a psychological bond that characterizes the connection of the individual to the organization.
The goal of this research was to know the commitment in the organization - affective, normative and instrumental- of the nurses performing tasks in a hospital centre and if this is in contact with personal variables that are related to the top management.
LITERATURE REVIEW
The organizational commitment can be considered fundamental to the practice of human resource management, then it gives the possibility to the organizations to know the perception and dedication of their employees.
Since the 70’s from the 20th century that studies on organizational commitment are frequent. The main reason given is related with the association of organizational commitment to outcome variables, such as, absenteeism, turnover, punctuality and behaviours of organizational citizenship3,4.
Literature shows that individuals committed to the organization exhibit less organizational withdrawal behaviours, such as absenteeism and turnover. It also shows that individuals with more levels of organizational commitment care more about punctuality and present an overall improvement ratio of individual performance7.
Other authors have also concluded that commitment will tend to benefit both worker and the organization8 by increasing performance, decreasing absenteeism and staff turnover.
The organizational commitment is considered a relative strength of the individual’s identification and his involvement in a certain organization9. This definition involves the concept of identification with the organization, namely, with values, mission and goals outlined by the organization.
In the 90’s arises a new definition of organizational commitment10 that refers to organizational commitment, like a psychological bond that characterizes the connection of the individuals to the organization. It is argued that the psychological commitment between the employee and an organization can take three different forms: when attitudes and behaviours are adopted, not because beliefs are shared, but simply to gain specific rewards; when an individual accepts influence in order to establish or keep a satisfactory relationship; when influence is accepted, because induced attitudes match with the individual’s own values.
So the multidimensional Meyer and Allen model of the organizational commitment arises. The dimensions of the organizational commitment of this model are designated as affective commitment, instrumental commitment and normative commitment11.
This model, which considers the organizational commitment as being composed of three components, each referring to different types of connections to the organization, has gained acceptance2.
The affective commitment represents a level in which the collaborator feels himself emotionally connected, identified and involved in the organization. Employees, who have a strong affective component, remain in the organization, because they want10.
This affective connection arises when the worker feels that the organization respects him and fairly supports him, relies on his superiors and on the organization, when he feels satisfied and accomplished in his work, when he feels that his personal and organizational goals match, and believes in the organization’s human values.
The developed model reveals an affective commitment’s component, which consists of the level in which the individual is psychologically connected to an organization through feelings like loyalty, affection, belonging, pleasure, protection12.
The affective commitment is based on an emotional connection to the organization, being likely that more people actually engaged are more motivated to contribute for the organization’s performance, have lower absenteeism, change less of organizations and adopt organizational citizenship behaviours13.
The normative commitment is based on reciprocity, reflects a feeling of obligation to continue in the organization. It is the belief of the worker's responsibility to the organization. This way of commitment is developed through experiences of familiar socialization and experiences of organizational socialization. Employees with a strong normative component remain in the organization, because they feel they should10.
The normative commitment tends to develop when the employee assumes the norms of the organization through socialization, receives benefits that lead him to reciprocally perform and establishes a psychological contract with the organization. It is possible that this contract takes place when one feels satisfied with the work, treated fairly and supported. The individual feels that the organization’s values are common to his personal values, relies on the leaders and considers that the organization adopts human resource policies that value the worker as a person and not as an instrumental resource13.
The instrumental commitment is associated with the costs related when the worker leaves the organization. Employees with a strong instrumental component remain in the organization, because they need10.
The instrumental commitment is acquired and increases when the employee recognizes, on the one hand, that if he abandons the organization he will lose all the investment made in it and, on the other hand, there is no choice to change the job to another organization. However when the worker feels unhappy, wronged, with no opportunities to develop his potential, when he performs a routine work without challenges it is likely that he establishes an instrumental connection.
Employees with a high instrumental commitment tend to have low motivation, lower levels of performance, and lower stimulus in order to resign and moderate levels of satisfaction and involvement with the work14.
The three components of organizational commitment should not be seen as unique types of commitment that characterize the commitment of a certain worker. On the contrary, workers can try each of these psychological conditions at different levels. For instance, a worker can feel both an extreme need and an extreme obligation to remain in an organization, but with no will to do it10.
So we can state that organizations are interested in promoting affective and normative bonds of their employees and decrease the instrumental bond. However so that this takes place it is necessary that organizations know the level of the organizational commitment of their workers and the variables that can determine it.
Several authors have focused on identifying the antecedents of the organizational commitment, that is, on identifying variables and factors that in some way determine that commitment15.
One can distinguish antecedents for the three components of the attitudinal commitment that were identified- affective, instrumental and normative1,16. So, antecedents of the affective connection to the organization are grouped into four categories: personal characteristics and characteristics of the function; work experiences; structural characteristics, giving more importance to the professional category and work experiences. The normative commitment is influenced by previous and later experiences to the individual’s entrance to the organization and by socialization experiences that stress the need to remain loyal to the organization. The instrumental commitment is developed based on investments made by the individual and on the perception of lack of alternatives.
There are demonstrative evidences that peoples’ management practices can encourage the adoption of attitudes and behaviors beneficial to the organization, as it is considered to be the organizational commitment. However it is accepted that commitment favors, among others, positive and productivity behaviors, has a unique interest in the current context, in which the relationship employee-employer has become more precarious and where employment is no longer seen as a job for life.
In a meta-analysis on the profusion of studies undertaken, 48 variables that somehow are related with the organizational commitment were identified and some of them can be considered antecedents, that is, variables can become the cause to the level of commitment. We can include here socio-demographic variables, work characteristics, characteristics of the organization and the type of relationship with the top managements. Also the leader’s communication and the type of leadership are described as being related to the organizational commitment7. Thus, although with some speculation, the same authors mention that a supervisor that provides appropriate and strict communication and that contributes with a good work environment will likely help to increase the commitment of the employees in the organization15.
In a study on health professionals, the author mentions the influence of the relationship with the top managements in the organizational commitment and in the affective, normative and instrumental commitment. The author considers the agreement with further references, that the relationships between employees and their supervisors or leaders can influence the commitment’s development, particularly in its affective dimension15.
Bearing these references in mind we can state that the top managements’ role and the relationships are needed to the collaborators’ organizational commitment.
METHODOLOGY
It is necessary to understand the different ways that commitment can adopt and the conditions that led to its development17.
Thus we intend to analyse the relationship between personal variables and the nurses’ organizational commitment under the affective, normative and instrumental dimensions.
This is a study of quantitative, descriptive and correlational nature with the purposes of: assessing the levels of commitment in the organization- affective, normative and instrumental- of the nurses in a hospital centre; analysing the influence of personal variables (age and gender) in the commitment in the organization- affective, normative and instrumental- of the nurses in a hospital centre; and analysing the influence of the relationship with the top management in the commitment in the organization- affective, normative and instrumental- of the nurses in a hospital centre.
The tool used to gather data was a questionnaire made up of three parts. The first part has closed questions related with personal variables. The second part of the questionnaire comprises items regarding the variable of the organizational commitment15. They are 16 items and correspond to the affective commitment (5 items), normative commitment (5 items) and instrumental commitment (6 items). The third part of the questionnaire regards to the variable relationship with the top managements and consists of 11 items15. Items are presented on a five-point Likert-type scale (1 corresponds to strongly disagree, 2 to disagree somewhat, 3 to neutral, 4 to agree somewhat, and 5 to strongly agree).
After formally presenting the project and the questionnaire to the ethic commission (Opinion 40-09/2011) and after the authorization by the direction of the hospital centre, the questionnaire was given to all nurses working between March and May 2011, period when the study was carried out.
The participation was volunteered and consented and the questions of anonymity and confidentiality were assured, according to the principles of research ethics. All nurses received the questionnaire. After the questionnaire was filled in the nurse put it inside an identified closed box with a slot. Putting the questionnaire did not require any identification, so no one who participated was identified.
The data were introduced and processed in a computer by using the statistical programme Statiscal Package for the Social Sciences (SPSS), versão 19 para Windows.
OUTCOMES AND DISCUSSION
654 questionnaires were delivered. 488 were received fully completed, being the response rate of 63.9%.
The majority (82.8%) of the 418 nurses who responded to this study is female. More than 60% are under 40 years of age. 277 (66.3%) are married or cohabit. 363 (86,8%) have a lasting connection with the institution (permanent contract).
The majority (82.8%) of the 418 nurses who responded to this study is female. More than 60% are under 40 years of age. 277 (66.3%) are married or cohabit. 363 (86.8%) have a lasting connection with the institution (permanent contract).
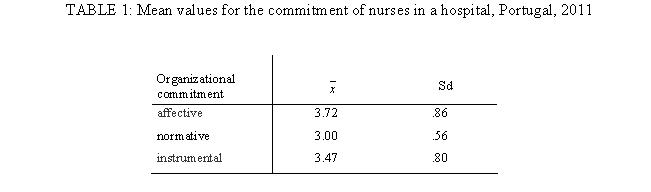
The average value of the affective commitment stands at 3.72 ±.86, in a 1-5 value scale, as shown in Table 1. Regarding the affective commitment according to age, we can see that its average value decreases from the group that is less 30 years old to the following group that is 30-39 years old, being this last group the one that achieves lower values (3.54 ± .85). It increases successively, achieving the highest average value in the group of 50 or more years of age (3.95 ± .86). The difference between the levels of the affective commitment on the age group, analysed by using the Anova One-Way test, revealed to be statistically significant [F(4,413)=3.068, p=.016]. These outcomes can be interpreted from the perspective that older workers have more positive work experiences than the younger, what will originate a bigger affective commitment in the organization17.
Age is, in different studies, positively related with commitment18. Other studies include this variable and the outcomes show a positive association with commitment, being this relationship stronger with the affective commitment than with the instrumental commitment7.
Female nurses showed a higher affective commitment (3.73± .86) than male nurses (3.66± .86). However this difference was not revealed when using the test t Student independent samples, for statistically significant. These outcomes can be considered in agreement with other authors, when they refer that women, especially the ones who are in an organization world ruled by men, are professionals strongly committed19. Nevertheless there is also agreement with studies previously performed, that show the lack of influence of the gender variable in the organizational commitment7,19.
The average value of the normative commitment stands at 3.00± .56, as shown in Table 1. Regarding the normative commitment according to age, we can see that its average value decreases from the group that is less 30 years old to the following group that is 30-39 years old, being this last group the one that achieves lower values (2.93± .52). It increases successively, achieving the highest average value in the group of 50 or more years of age (3,10 ± .64). The difference between the levels of the affective commitment on the age group, analysed by using the Anova One-Way test, not revealed significant differences.
The development of the normative commitment depends on the psychological contract established between the employee and the organization17. It can then mean that in the interactive process with the organization people train strategies over the years that facilitate the mutual adjustment.
Female and male nurses have shown a very similar normative commitment (2,99 ±.,56 e 3,02 ± .53). However, there are little confirmations of the relation in the commitment levels according to gender. Generically, it is indicated that there are no consistent relationships7.
The average value of the instrumental commitment stands at 3.47± .80, as shown in Table 1.
According to the instrumental commitment regarding age, we can see that its higher average value stands at group that is less 30 years old (3,65 ± .75). In the group with 50 or more years of age we can find the lowest average value (3,26 ± 0,81). The difference between the levels of the affective commitment on the age group, analysed by using the Anova One-Way test, revealed to be statistically significant [F(4,413)=3.331, p=.011].
Some studies describe age as being an antecedent variable of the instrumental commitment, but they draw attention to the necessary caution in the interpretation of that fact, since there might be overlapping of other variables like the professional category17.
Female nurses showed higher normative commitment (3.51± .78) than male nurses (3,30 ± .85). However this difference was not revealed when using the t Student test application for statistically significant independent samples.
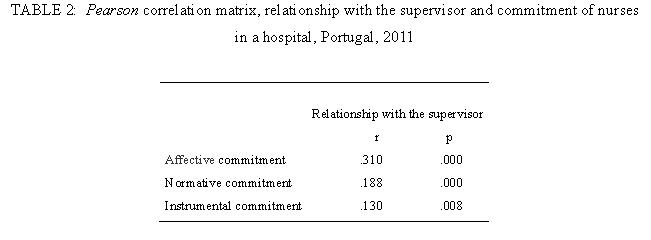
Regarding the nurses’ affective, normative and instrumental commitment and relationship with the top management, the Pearson’s correlation coefficient calculator enables to verify its statistical meaning. Although it is about low strength correlations, the value of the correlation between the relationship with the top management and the affective commitment is higher than in the normative and instrumental correlation, as shown in Table 2.
These outcomes meet the reference of several authors who refer that relationships between employees and theirs supervisors or leader can influence the commitment’s development particularly in its affective dimension7,17,18. Generically, the affective commitment in the organization is stronger among employees whose supervisors treat them with consideration and justice18.
Also in a study on nurses it was concluded that the relationship with the top managements was one of the predictor variables of the organizational commitment2.
In the managerial action, skills that integrate ethic-political and relational dimensions, based on the perspective that the transformation of the traditional management for a more flexible way of management does not imply the disappearance of power relationship, should be present20.
CONCLUSION
Different levels of commitment in the organization - affective, normative and instrumental- have been identified, according to the personal variables (age, gender) and its correlation with the relationship with the top management. The average value of the affective, normative and instrumental commitment stands at level 3 or above 3. The affective commitment is higher in the older age group and female nurses. The normative commitment is higher in the older age group and male nurses. The instrumental commitment is higher in the lower age group and female nurses.
A significant relationship between the affective, normative and instrumental commitment of the nurses and the relationship with the top management has been verified. The value of the correlation between the relationship with the top management and the affective commitment is higher than the value of the correlation with the normative commitment and the instrumental commitment. This means that nurses with a better favourable relationship with the top management are more engaged in the organization where they work, both in the affective’s or in the moral duty’s (normative) point of view, and have a bigger consciousness of the costs when leaving the organization. Thus we get to know the commitment in the organization- affective, normative and instrumental- of the nurses performing tasks in a hospital centre and its relationship with the top managements, answering to the formulated goal.
It is considered important that the top managements be aware of their relationship with the collaborators and they should instil more in the young nurses the goals of the organization, namely to the fulfilment of nursing care with an increasingly bigger level of quality and to the creation of a bigger identity with the organization.
One of the study’s limitation is the fact that only nurses were inquired, not including the opinion of the top managements. Other limitation has to do with the dependant variable and the independent variables that have been gathered at the same time. It is also necessary to include other independent variables in future studies.
Still it is a contribution to understanding the nurses’ organizational commitment.
REFERENCES
1.Camelo SH. Políticas de recursos humanos: sistema único de saúde, bases legais e implicações para a enfermagem. Rev enferm UERJ. 2009; 17: 589-94.
2.Frederico MM. Empenhamento organizacional de enfermeiros em hospitais com diferentes modelos de gestão: papel de variáveis de contexto. Referência. 2005; 1: 53-62.
3.Darden W, Hampton R, Howell R. Career versus commitment: antecedents and consequences of retail sales peoples’ commitment. Journal of Retailing. 1989; 65: 80-106.
4.Chen Z, Francesco A. Employee demography, organizational commitment, and turnover intentions in China: do Cultural differences matter? Human relations. 2000; 53: 869 - 87.
5.Farrell D, Peterson J. Commitment, absenteeism and turnover of new employees: A longitudinal study. Human Relations. 1984; 37: 681-92.
6.Porter L, Steers R, Mowday R, Boulian P. Organizational commitment, job satisfaction, and turnover among psychiatric technicians. Journal of Applied Psychology. 1974; 59: 603-9.
7.Mathieu J, Zajac D. A review and meta-analysis of the antecedents, correlates, and consequences of organizational commitment. Psychological Bulletin. 1990; 108: 171-94.
8.Reilly N, Orsak C. A career stage analysis of career and organizational commitment in nursing. Journal of Vocational Behavior. 1991; 39: 311-30.
9.Mowday R, Steers R, Porter L. The measurement of organizational commitment. Journal of Vocational Behavior. 1979;14: 224-47.
10.Meyer JP, Allen NJ. A three-component conceptualization of organizational commitment. Human Resource Management Review. 1991; 1: 61-89.
11.Allen NJ, Meyer JP. The measurement and antecedents of affective, continuance and normative commitment to the organization. Journal of Occupational Psychology. 1990; 63: 1-18.
12.Jaros S. An assessment of Meyer and Allen’s: three-component model of organizational commitment and turnover intentions. Journal of Vocational Behaviour. 1991; 51: 319-37.
13.Rego A, Cunha M, Souto S. Espiritualidade nas organizações e empenhamento organizacional: um estudo empírico [documento de trabalho em gestão]. Aveir (PT): Universidade de Aveiro; 2005.
14.Saunders M, Thornhill A. Forced employment contract change and the psychological contract. Employee Relations. 2006; 28: 449-67.
15.Ferreira MM. Empenhamento organizacional de profissionais de saúde em hospital com diferentes modelos de gestão[tese de doutoramento]. Braga (PT): Universidade do Minho; 2005.
16.Meyer JP, Allen NJ, Smith C. Commitment to organizations and occupations: extension and test of a three-component conceptualisation. Journal of Applied Psychology. 1993; 78: 538-51.
17.Meyer JP, Allen NJ. Commitment in the workplace. London (UK): SAGE Publications. 1997.
18.DeCotiis T, Summers T. A path analysis of a model of the antecedents and consequences of organizational commitment. Human Relations; 1987; 40 (7): 445-70.
19.Jardim R. Empenhamento organizacional afectivo e saliência das actividades – diferenças entre sexos [dissertação de mestrado]. Lisboa (PT): Universidade de Lisboa; 2010.
20.Paiva SM, Silveira CA, Gomes EL, Tessuto MC, Sartori NR. Teorias administrativas na saúde. Rev enferm UERJ. 2010; 18: 311-6.