NA = no answer
RESEARCH ARTICLES
Nurses' organizational commitment in a hospital in Portugal: analysis of the impact of organizational restructuring
Maria Manuela Frederico-FerreiraI
IPh.D. in Business Sciences, Post-Doc in Business Sciences. Coordinating Professor of the Nursing School of Coimbra, Quality and Assessment Board. Coimbra, Portugal. Email: mfrederico@esenfc.pt
DOI: http://dx.doi.org/10.12957/reuerj.2015.12279
ABSTRACT
Organizational restructuring often has impact on collaborators' behavior. This exploratory, descriptive, correlational study examined the impact of restructuring processes on levels of organizational commitment among nurses, to assess whether levels differ before and after the restructuring process, and provide recommendations and/or suggestions for enhancing organizational commitment. Data were collected by questionnaire in 2011 from the sample of 158 nurses who experienced the process of organizational restructuring and thus can give opinions about changes in relations with the institution. The information provided on changes in the hospital and the effect these changes might have was considered insufficient by a considerable proportion of the participants. These findings highlight the nurses' diminishing normative and affective relations with the organization.
Keywords: Loyalty; nurses; hospital restructuring; organizational commitment.
INTRODUCTION
The study of organizational behavior has shown that human behavior in the organizations is influenced by situational and individual characteristics, and that factors can be created to motivate or induce the individual to adopt a certain behavior or attitude. In other words, factors have been created that lead the individual to act in a particular way1, aligning the personal interests with those of the organization.
The current global changes and the organizational restructuring of health services in different countries, often resulting from imposed policies, affect nursing services2.
Nurses represent a significant percentage of the human resources allocated to health institutions, mainly hospital institutions3, and are strongly targeted in organizational restructuring processes.
The objectives of this study were to assess the impact of the restructuring process on the nurses' organizational commitment; to assess whether there is a difference between the levels of organizational commitment before and after the restructuring process; and to provide some recommendations and/or suggestions, with the aim of improving organizational commitment.
LITERATURE REVIEW
Organizational commitment, which can be defined as the psychological state that characterizes the employees relationship with the organization, seems to be a good indicator of the reconciliation of those interests, since it is a predictor of the behavioral intentions of the employees4. The interest in this construct is based on the assumption that it is associated with important variables for increasing organizational effectiveness and productivity 5. Along the same line of reasoning6, in theory, organizational commitment influences several behaviors which are important for the smooth functioning of organizations, such as the workers' intention to stay in the organization, to make efforts to advance it, and to deliver a good performance. The interpersonal relationships should also be considered, because employees consider the respect and trust from their leaders as a key factor in the relationship7.
The components of organizational commitment, particularly the affective (based on an emotional bond to the organization) and the normative components (based on reciprocity, reflecting feelings of obligation to remain with the organization) should not be seen as unique types of commitment that characterize an employee's commitment. We should rather consider that workers can experience each of these psychological states at different levels.
Organizations have an interest in promoting the affective and normative ties of their employees, but they first need to know their level of organizational commitment and the influencing variables3.
Organizational policies that emphasize profitability and rationalization, the development and merit of the professionals, and the granting of incentives, are characteristics of the hospital management models, but can also impact the workers' commitment.
Nursing, as a professional group, is strongly targeted by the change and restructuring processes occurring in health institutions. The studies focusing on the effects of health reforms in the nursing profession address a diverse set of issues, essentially structured around themes related to the changes in the professional culture and roles8,9.
The consequences of the restructuring process and the challenges are evident both in clinical practice and in the management and workload of nurses. In the area of management, nurses' power of intervention in the hospital administrative functioning decreases. With regard to the workload, the increased number of tasks could lead to a change in the professional roles and in the delegation of less specialized tasks to other professionals with lower qualifications.
These changes alter the work organization itself, which may translate into a simultaneous presence of Fordist and post-Fordist models of work organization. Indeed, some techniques of the new public management coincide with the Fordist practices, such as increased routinization, deskilling and management control over the work process9,10, while others are similar to the post-Fordist practices, such as flexibility, versatility and mobility9.
METHODOLOGY
This project is mainly an exploratory study, with the following objectives: to assess the impact of the restructuring process on the nurses' organizational commitment; to assess whether there is a difference between the levels of organizational commitment before and after the restructuring process; and to provide some recommendations and/or suggestions with a view to improving organizational commitment. The approach is predominantly quantitative, descriptive and correlational.
The data collection instrument used was a questionnaire consisting of four pages and three groups of questions. The first group, with open-ended and closed-ended questions, focused on the information provided in the change process and the changes in the relationship with the institution. In each closed-ended question, the participants in this group were asked to justify their choice. The introduction to the questionnaire, in addition to presenting and framing the study, explained the meaning assigned to 'changes in the hospital': When we talk about 'changes in the hospital', we mean the transition from a SPA hospital (Administrative Public Sector) to an EPE hospital (Public Business Entity). The second group included 40 statements on the affective, normative and continuance commitment and the perceived organizational support, and used a Likert-type scale (from 1 to 5, where 1 is ...strongly disagree..., 2 ...disagree somewhat..., 3 ...neutral..., 4 ...agree somewhat..., and 5 ...strongly agree...). The third group included questions on biographical data.
The variable organizational commitment is based on the Organizational Commitment Scale11,12, which has already been validated and applied to health professionals in Portugal13.
After the formal procedures for submitting the project and the questionnaire to the Ethics Committee (Opinion No. 40-09/2011) and obtaining permission from the hospital's board of administrators, the questionnaire was distributed to each nurse in an envelope to be closed after completion. The process of questionnaire distribution and collection occurred in 2011.
Although nurses are the subjects of the analysis, for the purposes of this study, the nurses had to work in a hospital institution where the management model had been restructured. Thus, the nurses in this sample worked in hospitals which underwent a management restructuring in 2005. The nurses consented to the voluntary participation in the study and the issues of anonymity and confidentiality were ensured, according to the ethical research principles. The questionnaire was delivered in an individual envelope that nurses should close after completion and deposit in an urn box without any identification of the questionnaire respondents.
Quantitative data were processed using the statistical software Statistical Package for the Social Sciences (SPSS), version 19 for Windows, in which the descriptive statistical analysis was performed. The content analysis technique was used in open-ended questions.
A total of 723 questionnaires were delivered: 53 were returned blank, i.e. unfilled, four were incomplete and 502 were not returned. A total of 164 questionnaires were duly completed and, therefore, were considered valid to be used in the study, representing a response rate of 22.7%.
Six nurses reported that they did not work at the hospital before it was an EPE hospital. Thus, their answers were not included in the data from the first group of questions, because it concerned the process of change and the nurses' opinions on how their relationship with the institution changed.
This analysis took into account the 2011 study and some comparisons with the results obtained from a study carried out in 2002, which used the same measuring instrument that was used in 2011.
RESULTS AND DISCUSSION
In 2011, the sample was mostly composed of women - 135 (82.4%) female nurses. The most representative age group was 30-39 years - 79 (48.2%) nurses. The most represented professional category was nurse level I (initial level of the nursing career) with 114 (69.7%) nurses, followed by 30 graduate nurses (18.3%) and 27 specialist nurses (16.4%). Fifty-four (33.1%) nurses who completed the questionnaire worked in the organization for less than 10 years.
Information about the changes
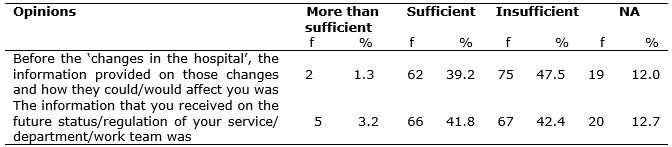
Before the changes in the hospital, 75 (47.5%) participants considered the information provided on these changes and how they could/would affect them to be insufficient, as shown in Table 1.
TABLE 1:
Opinions of the nurses regarding the information provided on the organizational restructuring. Portugal, 2011. (N=158)
NA = no answer
Communication and information processes are necessary strategies for leaders, by enabling the understanding of the information and providing a means of interaction between people and the exchange of views. The bond can be formed through the recognition and understanding of points of view, creating exchanges of subjective perspectives.7
A total of 53 justifications were presented, with 48 of them being from nurses who considered the information to be insufficient. These justifications were related to the lack of information, the need to understand the change, to be integrated as an active member in the process, and to feel motivated for the change, as illustrated by the following excerpts:
There was no information. (E7)
The organization should have informed us about the changes that were going to take place. (E35)
No type of information was provided. What will change? What are the immediate consequences for the staff and service? (E74)
Only the information that would allow us to understand what was going to change. (E91)
I'm still a bit unfamiliar with the changes that occurred, it would be important to have a debriefing session with the professionals […]. (E13)
[…] information that would allow us to understand what was going to change. […]. (E123)
There was no information at all provided directly by the organization. It was only through the social media that we had any knowledge of the situation. (E19)
Although the justification was only requested if the nurse considered the information to be insufficient, five nurses who considered the information to be sufficient justified their answer. The following excerpts allow us to understand the justifications:
There was a debate session in a room where the changes were explained. (E4)
There was a previous meeting with nurses. (E27)
I remember that we had a meeting with the Director Nurse, where he explained it very well: if we did not sign with the EPE, we would leave the hospital (at the time I had a fixed-term contract). (E56)
As it was an essentially political decision, it was basically decided overnight and without public discussion." (E78)
I didn't notice any change. In fact, I also have no interest in how it should be. I think that the patients receive the necessary care, regardless of who is managing it. (E141)
According to Table 1, the information which nurses considered to have received on the future status/regulation of their service/department/work team was considered insufficient by 67 (42.4%) participants, but sufficient by 66 (41.8%) participants.
We asked them to justify their answers and, in case they considered the information received to be insufficient, to mention the type of information that they should have received. Thirty-six justifications were given. Such justifications reflected the need for information in order to adapt to change, to reduce uncertainty, and to be aware of the implications for employees, as illustrated by the following excerpts:
There was no information whatsoever. There were changes in the contracts - changes in the teams because of the increase in the number of hours. The practices remained the same. (E20)
We can only adapt to change if we receive clear information. They have to provide us with knowledge, skills; they have to motivate us to have a better performance. (E47)
I didn't notice any changes in the work team that are related to the changes in the hospital. (E90)
The changes that occurred were an initiative of the work team in order to improve the care provided and to respond to the increase in the number of patients in this unit. (E105)
There is great uncertainty in my workplace as to what will be the future of the medical specialties in my service. This information was not provided. (E74)
What changes? Advantages/disadvantages? (E123)
I felt no changes in how the services function, but the information on the future status was scarce. The feeling was: 'wait and see!' I was informed that I would start working 40 hours a week and receive a remuneration equivalent to that workload increase. (E39)
The regulations are obscure or inexistent. The changes have not improved the few procedures/rules/regulations that existed. (E53)
What status? The regulations are the same. There were basically no changes […]. (E91)
[…] the changes should have at least been published in an internal bulletin. (E19)
Information about the negative implications for the workers. (E66)
I continued to perform the same tasks […]. (E25)
The legal and administrative changes and the extent to which these changes are related to the workers' future. (E74)
I didn't notice and I wasn't informed of any change in the regulation, […]. (E101)
Everything. After all the hospital operates thanks to the staff! (E74)
Nine nurses who considered the information to be sufficient also gave their justifications, as can be seen in the following excerpts:
It was sufficient, because the information was gradually provided; I believe that the changes were seen later and gradually. (E4)
Within the service, the information was sufficient. It was mainly provided by my immediate superior. (E27)
The information was enough, although it was not discussed with the team. […]. (E45)
The information was obtained when questions were asked. (E103)
The information received was enough for the situation. (E78)
Classification of the nurses' relationship
Several studies mention that the relationship between employees and their supervisors or leaders can influence the development of organizational commitment. Studies show that the affective commitment is stronger among employees whose supervisors treat them with respect and fairness14, that the relationship with senior managers is one of the predictive variables of organizational commitment15, and that the nurses become more committed to the organization, both from the affective and normative perspectives, and are even more aware of the costs involved in leaving the organization, when there is a more positive relationship with the leaders 3. Indeed, the employees' behaviors are influenced by their beliefs regarding the extent to which the organization values their collaboration; hence it is important to develop a workplace culture and a positive sense of the organization16.
Although a high percentage of nurses considered their affective relationship with the hospital as average, both before and after the changes, it should also be mentioned that, before the changes, 33 (20.9%) nurses considered this relationship to be high, and that, after the changes, only 13 (8.2%) nurses continued to consider it as high, as shown in Table 2.
TABLE 2:
Classification of the relationship between the nurses and the organization. Portugal, 2011. (N=158)
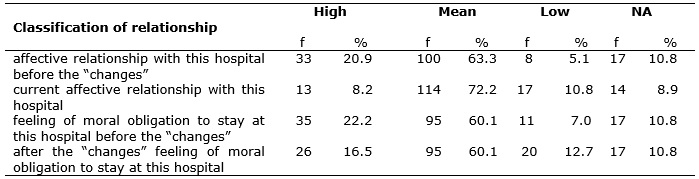
As for the sense of moral obligation to stay in that hospital, the largest percentage of nurses considered it to be average before and after the changes (60.1%). However, before the changes, 35 (22.2%) nurses considered it to be high, whereas, after the changes, this group was reduced to 26 (16.5%) nurses, as according to Table 2.
If the interviewees stated that their relationship of obligation to the hospital changed after the restructuring, we asked them to provide a reason for that. Eighteen nurses answered, focusing on recognition, fairness and appreciation of people, as illustrated by the following excerpts:
We have lost the spirit of mutual aid, we are each in our workplaces and we are distant from the other colleagues […]. (E91)
The lack of consideration with which people are treated. (E13)
I'm not satisfied […] with the lack of recognition for my performance. (E35)
[…] I currently feel no obligation because we feel that we are dispensable and easily replaced. There is no appreciation for the investment being made […]. (E52)
Because the number of employees has increased and because people don't know each other. (E66)
Perhaps the lack of interest from those in charge for the hospital to captivate people. […]. (E74)
Personal demotivation for the lack of recognition of the work being performed. (E116)
Loss of character of the institution, distancing and depersonalization. (E123)
At this moment, I still feel the moral obligation to fulfill my duties well and promote the image of the institution to which I belong. Affectively, things have changed a little, the relationships between the team members have changed, for the worse, perhaps due to the pressure and overload brought about by the changes and the restructuring. (E91)
Feeling of injustice; equality of classes; a more rigid hierarchical structure; less autonomy. (E134)
Providing careers within the company, where there is progression, objectives, […]. (E116)
I kept the same relationship because I love my profession and I have quality resources available to do my job […]. (E90)
Most of the nurses (70.9%) mentioned that the relationship between the administration and the employees remained the same after the changes; however, 15.8% considered it to be worse than before.
The answers to the questions: what has changed? and what do you think could be done to improve things? reflected a sense of alienation/closeness, which was illustrated by the following excerpts:
The administration […] distanced itself from the reality of the services; […]. (E35)
More arrogance; less closeness; less accessibility. (E90)
It seems to me that the administration is unaware of the reality of the services and the difficulties that we, the employees, experience while performing our duties to the best of our abilities. (E105)
Change the people who are in charge. They need more sensitivity and less authoritarianism. (E138)
The relationship between the administration and the employees is distant. (E66)
[…] The only way to change is through a better relationship between those involved, but first both parties have to want it. (E74)
Changing the institutional policies. (E20)
More recognition of the effort and zeal demonstrated by my performance. (E116)
Comparison of values: organizational commitment
In the 2002 study, the sample was composed of 161 nurses, out of which 126 (78.3%) were women. The most common age groups were composed of nurses aged up to 30 years - 60 (37.3%) nurses, and between 30 and 39 years - 61 (37.9%) nurses. The most represented professional category was graduate nurses - 72 (44.7%) nurses, followed by the categories of nurse level I - 64 (39.7%) nurses, and 25 nurse specialists (15.5%). In addition, 105 (65.1%) nurses who completed the questionnaire worked in the organization for less than 10 years.
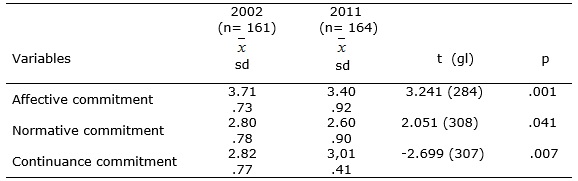
Affective commitment and normative commitment13,15,16 had lower mean values in 2011 than in 2002. In turn, instrumental commitment 13,15,16 showed higher mean levels in 2011 than in 2002. The differences in the mean scores were statistically significant, as shown in Table 3.
Table 3:
Comparison of organizational commitment scores in 2002 and in 2011. Portugal, 2011.
Indeed, before the changes, 33 (20.9%) nurses considered their affective relationship with the hospital to be high, whereas only 13 (8.2%) nurses considered it to have remained high after the changes. The sense of moral obligation to stay in the hospital was also high before the changes for 35 (22.2%) nurses, whereas this group was reduced to 26 (16.5%) nurses after the changes, according to Table 2.
As an indicator with less positive effects in organizational performance, the instrumental commitment was expected to show a low mean score, but this was not the case. This score surpassed the normative commitment score, and there was even an increase when comparing 2002 with 2011. Thus, this is an indication that the reason for maintaining the connection to the organization is increasingly related to the costs (e.g., lack of alternatives) incurred by the employee when leaving the organization.
In the comments field, the nurses made reference to their hope that the conclusions of this study would be disclosed, as the following statements show:
I hope that this questionnaire has some impact and helps overcome some of the difficulties felt in the services. (E20)
They have to value the people who work at this institution. […]. (E138)
I wish that the hospital administrators would become aware of what is really happening in the daily life of the staff in this hospital; […]. (E35)
CONCLUSION
The changes occurring in the organizations call for the important need to assess and understand the workers' behavior, their opinions and, particularly, their organizational commitment.
The information provided on the changes in the hospital and on how these changes could affect them was considered insufficient by a significant percentage of nurses - 78 (47.5%) nurses. They justified it by saying that there was a lack of information, that they needed to understand the change and be integrated as active members in the process, and that they should feel continuously motivated to change.
The decrease of the affective and normative relationships between the nurses and the organization in both moments of the study is clear, with the mean differences in affective commitment being statistically significant.
The contributions of this study are the assessment of the impact of the restructuring process on the nurses' organizational commitment and the findings regarding the existence of differences in the levels of commitment before and after the restructuring process. Taking into account the necessary caution as with any type of generalization, the results of this study can be projected to other health institutions undergoing restructuring processes.
As recommendations to improve the organizational commitment, and based on the suggestions given by some participants, the administrators and managers must take the proximity and the information to the employees as a decisive aspect for the identification with the organization, given the fact that commitment promotes positive behaviors, well-being, motivation and productivity, among others.
This study is not free from limitations, although these did not influence the results. Some limitations include the low response rate, the fact that only nurses were interviewed, and the fact that the opinion of the organization's managers was not considered. It must be added that, although we excluded the respondents who did not work at the institution before the restructuring process, this was not a paired study, which would be ideal in comparative terms.
REFERENCES
1.Aas I. Incentives and financing methods. Health Policy.1995; 34.205-20.
2.Camelo SH. Políticas de recursos humanos: sistema único de saúde, bases legais e implicações para a enfermagem. Rev enferm UERJ. 2009; 17:589-94.
3.Ferreira M, Silva I. Empenhamento organizacional de enfermeiros e relação com a chefia. Rev enferm UERJ. 2013; 21:156-61.
4.Iverson R, Roy P. A causal model of behavioural commitment: evidence from a study of Australian blue-collar employees. Journal of Management. 1994; 20:15-41.
5.Hunt S, Morgan R. Organizational commitment: one of many commitments or key mediating construct? Academy of Management Journal.1994; 37:1568-87.
6.McCaul H, Hinsz, V, McCaul D. Assessing organizational commitment: an employee's attitude toward the organization. The Journal of Applied Behavioural Science. 1995; 31:80-90.
7.Vieira TP, Renovato RD, Sales CB. Compreensões de liderança pela equipe de enfermagem. Cogitare Enferm.2013; 18:253-60.
8.Davies C. Competence versus care? Gender and caring work revisited. Acta Sociologica.1995; 38:17-31.
9.Walby S, Greenwell J, Mackay L, Soothill K. Medicine and nursing: professions in a changing health service. London (UK): Sage Publications; 1994.
10.Daykin N, Clark B. They'll still get the bodily care. Discourses of care and relationships between nurses and health care assistants in the NHS. Sociology of Health & Illness. 2000; 22:349-63.
11.Meyer J, Allen N. A three-component conceptualization of organizational commitment. Human Resource Management Review. 1991; 1: 61-89.
12.Meyer J, Allen N. Commitment in the workplace. London (UK): SAGE Publications; 1997.
13.Ferreira MM. Empenhamento organizacional de profissionais de saúde em hospital com diferentes modelos de gestão [tese de doutoramento]. Braga (Pt): Universidade do Minho; 2005.
14.DeCotiis T, Summers T. A path analysis of a model of the antecedents and consequences of organizational commitment. Human Relations. 1987; 40: 445-70.
15.Frederico MM. Empenhamento organizacional de enfermeiros em hospitais com diferentes modelos de gestão: papel de variáveis de contexto. Referência. 2005; 1:53-62.
16.Frederico-Ferreira M. Percepção de suporte organizacional em hospitais públicos: estudo em enfermeiros. Análise Psicológica. 2008; 4:697-706.