ORIGINAL RESEARCH
Sexual violence: from complaint to criminalization of offenders
Daniele Ferreira AcostaI; Cristiane Lopes AmarijoII; Camila Daiane SilvaIII; Vera Lúcia de Oliveira GomesIV; Cristine Coelho CazeiroV
I
Nurse. PhD in Nursing. Associate Professor of the Nursing School of the
Federal University of Rio Grande. Member of the Group for Studies and
Research in Nursing, Gender and Society. Rio Grande, Brazil. E-mail: nieleacosta@gmail.com
II
Nurse. PhD Student in Nursing, Graduate Nursing Program, Federal University
of Rio Grande. Member of the Group for Studies and Research in Nursing and
Health. Rio Grande, Brazil. E-mail:
cristianeamarijo@yahoo.com.br
III
Nurse. PhD in Nursing. Associate Professor of the Nursing School of the
Federal University of Rio Grande. Member of the Group for Studies and
Research in Nursing, Gender and Society. Rio Grande, Brazil. E-mail: camilad.silva@yahoo.com.br
IV
Nurse. PhD in Nursing. Professor of the Nursing School of the Federal
University of Rio Grande. Member of the Group for Studies and Research in
Nursing, Gender and Society. Rio Grande, Brazil. E-mail: vlog1952@gmail.com
V Nurse. Master Student at the Graduate Program in Public Health of the
Federal University of Rio Grande. Rio Grande, Brazil. E-mail: ccoelhoc@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.11518
ABSTRACT
Objective: to characterize police complaint reports and establish the dimensions profile the forensic medical examination of victims of sexual violence. Method: this retrospective study analyzed occurrences of sexual violence against women 18 or more old, recorded at a Special Police Service for Women. Data were collected using a tool adapted to Microsoft Excel®, and analyzed using descriptive statistics. Results: time between assault and complaint ranged from hours to fourteen months. Most victims who underwent forensic examination were young, white and had attended middle school. Most offenders were unknown, older men with less schooling than their victims. Women abused by men they knew withdrew the complaint. Conclusion: for effective care that offers a solution, it is not enough to implement interdisciplinary actions; services must accept and support women on the basis of humanized care.
Keywords: Sexual assault; woman's health; gender; intersectorality.
INTRODUCTION
Violence against women has been characterized by the World Health Organization (WHO) as a global public health problem of epidemic proportions1. Among the different types there is sexual violence, which goes beyond cultural barriers, social classes and socioeconomic levels and may occur in the private space and in the public sphere2. This type of violence is characterized as a brutal way of violating human, sexual and reproductive rights of women, and as a manifestation of male dominance over women3.
Thus, there is the need for multidisciplinary and intersectoral assistance to victims, with coordinated actions between legal, police, psychosocial and health services. However, not all employees feel able to take action in situations of violence against women. The main problems faced relate to the lack of approach of this phenomenon during graduation or even due to the institutional work dynamics that fails to promote intersectoral work4,5.
Because of this, in the police area, actions are generally centered on the realization of the police report. In the health field, efforts are focused on the consequences of violence, through medicalization and referral to the police station6 or to the psychologist4, thus transferring the responsibility for the 'solution' of cases. Soft technologies become secondary in victim assistance, weakening their coping process.
Having in mind that health services are the gateway to the network support and that the municipality has a Specialized Police Service and a reference hospital in the handling of cases of sexual violence, it is important to know the epidemiological situation of this type of violence in the city.
So, this study aims to characterize the records of police reports and measure the achievement of forensic examination of victims of sexual violence in the city of Rio Grande/RS. Authors believe that this study may contribute to the improvement of multidisciplinary actions and interventions targeted at women suffering such violence.
LITERATURE REVIEW
The woman is subjected to sexual violence when a person using physical force, coercion or psychological intimidation forces her to practice, maintain or witness sexual acts that she does not want to share. We can also include in this description unwanted fondling, compulsory exposure to pornography, forced prostitution and partner's refusal to use condoms1. According to Law 12,015 of 2009, crimes against sexual dignity consist of rape, sexual harassment and sexual violation by fraud7.
These acts grounded in authority conflicts, in power and relationships, and destruction of women are supported by the macho culture3 and disseminated, often implicitly, especially when committed by an intimate partner.
A data collection on women's health and domestic violence conducted by WHO in ten countries8 showed that 15% to 71% of women have experienced physical or sexual violence by a spouse. In Brazil, in 2011 alone, there were 12,087 cases of rape9. Although the data are alarming, they do not show the reality of the facts, since only 10% of cases of sexual violence are reported9.
This underreporting is justified by the constraint of women in exposing the situation to others, the by the lack of credibility of the legal system and by fear of confrontation with the offender2. There are also women who give up on the complaint by emotional dependence on the partner and to keep the family together. Cultural issues also contribute to the invisibility of the phenomenon. In countries like India marital rape is not considered a crime, which results in low rates of complaints10.
Given these findings, it is clear the impact of violence on the victim's health-disease process, which triggers, directly or indirectly, physical and psychological problems, including cases of depression, panic attacks and anxiety11. In the field of sexual health, victimized women are more vulnerable to unwanted pregnancies, sexually transmitted diseases, abortion and gynecological disorders1,9. They can also present vague complaints that do not constitute a diagnosis alone. As a result, they have most need of care in health services1.
In order to guide the professional assistance, the Ministry of Health launched the Technical Standard for Prevention and treatment of injuries resulting from sexual violence and listed the aspects related to assistance to women, awareness of staff and human and physical resources necessary to meet them11. It also pointed out the importance of health professionals reporting the signs of violence during care for the victim, highlighting the need for detailed description or photography of physical, genital or extra-genital damage because such records may serve as evidence in the police investigation11.
Another way to raise evidence of violence is the forensic examination, held at the Medical Legal Institute (MLI). Medical and legal findings are critical for both proving the fact and for the identification and the criminalization of the offender12. However, the forensic examination is only carried out when the offender is denounced through a police report. It is common that health services require this document to meet the victim of violence, but this is an incorrect and illegal requirement11.
METHODOLOGY
This is a documental, retrospective, exploratory-descriptive study with quantitative approach performed in the Specialized Police Service to Women (SPSW) of Rio Grande/RS. Authors analyzed police incidents recorded between August 2009, when the service was inaugurated, and December 2011. The sample of this study were all the police occurrences relating to sexual violence against women aged 18 years or older and that were included in the archives of SPSW in the period of data collection, that is, between October 2011 and March 2012, totaling 39 occurrences.
Data were collected directly in a laptop computer through an instrument adapted to the Microsoft Excel®. This instrument contained data from the victim, the offender, the type of violence, the description of the violent act and the outcome of the complaint. For the analysis, researchers used descriptive statistics. The study met the Resolution No. 466/12 and the project was approved by the Research Ethics Committee in the Health Area of the Federal University of Rio Grande under opinion 137/2011 and Presentation Certificate for Ethics Assessment (CAAE) No. 23115004017/2011 -03.
RESULTS AND DISCUSSION
Presentation of results begins with a brief description of the 39 police complaints of sexual violence recorded at the SPSW, in the selected period. Subsequently, the aspects of the 22 forensic examinations are exposed, as well as the profile of those involved in the violent act.
Unveiling the violence suffered
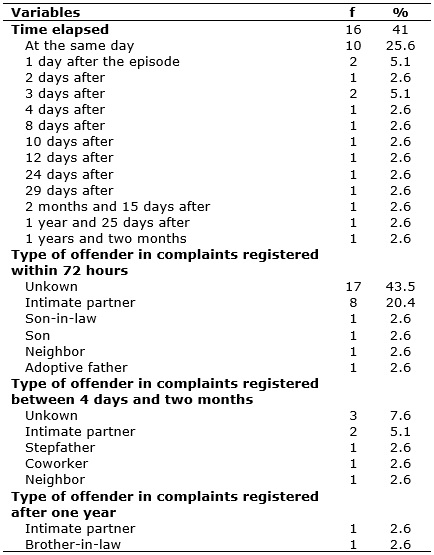
It was found that the time elapsed between the sexual crime and the complaint ranged from a few hours up to 1 year and 2 months. Moreover, it was possible to correlate this data with the degree of relationship between victim and offender, as shown in Table 1.
Of the 29 victims who registered the complaint within 72 hours, 43.5% were raped by an unknown person; 20.4% by an intimate partner and the others by family members. In 7.6% of cases the police incident report occurred between four days and two months, having a stranger as the main accused. In both cases the victims took over a year to carry out the complaint.
TABLE 1:
Distribution of cases of sexual violence according to the time elapsed
between the violent act and the realization of the complaint and type of
offender. Rio Grande/RS, 2012. (N=39)
Other research in Women's Police Stations show that the main form of reported violence is physical13 and psychological14,15. Although this study address only sexual violence, according to the literature it is common the association of different aspects of violence, and in cases of sexual violence the use of physical force and threat are often present12,16.
The type of violence seems to be related to the relationship between aggressor and victim, according to data from this and other research. In cases of physical and psychological violence, the aggressor, in most cases, is the partner14,15. In this study, which only portrays sexual violence, 51.3% of the offenders were unknown to the victim. Thus, one can infer that when it comes to sexual crime against adult women, men outside the family life are the majority among the offenders. Such mention is strongly grounded by other results that report as the main aggressor in cases of sexual violence a stranger13,16,17 or other men than the spouse14.
When sexual violence is perpetrated by a partner, it has many beliefs and taboos. Resulting from the dominant gender culture, some women believe they should meet their husbands' needs, which reflects on the low perception of such duress within marital relationships18. Survey of the Brazilian population has shown that 14% of respondents said they completely agree and 27.2% totally or partially agree that a married woman must meet her husband in bed, even when she has no desire19. Such representations end up veiling the reality of such violence when committed by partners, resulting in fewer reported cases.
By analyzing the time elapsed between the violent act and the record of police report, 74.3% of women made the complaint within 72 hours after the assault. Of these, 43.5% were victimized by someone they did not know. Moreover, of the 20.5% occurrences recorded within four days and two months, in 12.9% the offender was the partner or someone the victim knew. The two complaints made after one year referred to the partner and a brother-in-law.
Thus, in this study, it appears that the absence of bond seems to be a facilitator to the complaint before the positive association between kinship with the offender and long time elapsed between the violent act and the police report.
Profile of victims
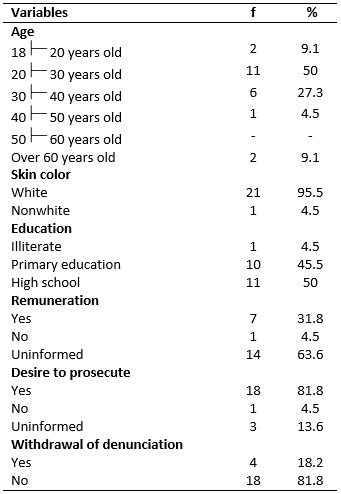
Soon after the formalization of police report, 22 (56.4%) women underwent forensic examination for the purpose of obtaining criminal evidence. In 17 (77.3%) cases, the examination was performed by male doctors and in 4 (18.2%) by female doctors. The remaining occurrences did not have this data. The age ranged between 18 and 68 years, with a predominance of the age group between 20 and 30 years (50%). Most women were white and had completed high school. With respect to remuneration, 31.8% had a source of income. When they made the police report, 18 (81.8%) wished to take legal action against the offender. However, 4 (18.2%) victims chose to give up the complaint.
TABLE
2:
Distribution of cases of sexual violence according to the profile of
victims and the characteristics of the police report. Rio Grande/RS, 2012.
(N=22)
Forensic findings are essential as criminal evidence against the offender. However, only a small portion of the victims hold the examination in the proper time to collect evidence12. International study highlights the emotional impact, the fear of the forensic examination and social vulnerability as issues that hinder or delay the completion of that examination20.
In cases of sexual assault with penetration, the Ministry of Health recommends that early treatment with antiretroviral drugs and emergency contraception occurs within 72 hours of violence since after this period the drug significantly loses effectiveness by providing less protection 11. In this sense, breaking the inertia and barriers resulting from shame, fear and guilt are essential so that health problems are minimized. It is also emphasized the importance of professionals in the police stations orientate the victims about their right to undergo forensic examination, as this is the main institution to refer them to the MLI21.
If the forensic examination is not performed directly in the MLI, experts can make the forensic report based on medical records, when the woman had sought a health service11. Therefore, it is essential that the professional who attended the victim becomes aware of the importance of detailed record of the physical conditions of the victim11. This does not make way for a technical care but must be part of a warm and humanized care. Moreover, in order to facilitate intersectoral coordination, it is necessary that health professionals, legal professionals and the police know the process of communication between the services, its assignments and the role of the network for combating violence against women5.
In this study, of the 22 women who underwent the referred examination, 17 (77.3%) were seen by a male professional. According to Law No. 8,862, of March 28, 1994, the forensic examination should be performed by two official experts, and in the absence of these, it can be achieved by two reliable people that have higher education; preferably with technical qualifications related to the nature of the examination22. Therefore, although the law does not talk about the gender of the professional, the fact of having to expose the body to the opposite sex may represent a barrier to the realization of forensic examination.
Regarding the profile of the victims, most were between 20 and 30 years old, were white and had complete or incomplete high school. Surveys show that young women are the most vulnerable to different types of violence13,17. When analyzing the profile of victims of sexual violence alone, the results, unlike this study, point to the predominance of younger women, averaging 19 years23 or less3,17.
Schooling had a low rate of change, and 50% of victims had complete or incomplete high school and none had higher education. According to the literature, women reporting violence often have a homogeneous profile, are from lower class, have low educational level, have predominantly complete or incomplete primary education and work as housekeepers24.
Regarding the remuneration, 7 (31.8%) women had some income. The fact that 63.3% of police reports have not included this data hampers further discussion and reinforces the need for detailed and complete filling of the records so that epidemiological data are traced and thus reversed in public policies and targeted care. As observed in this study, the dimensioning of violence against women is limited because of the inadequate completion of legal sources and lack of information, which ends up masking the real magnitude of the problem25.
Most victims who conducted the forensic examination proceeded with the complaint against the offender. It is noteworthy that 13 (59%) offenders were unknown for the victims and 4 (18%) were intimate partners. The four women who dropped out of the complaint were victimized by the neighbor, intimate partner, son and the adoptive father.
Profile of perpetrators
Data regarding the profile of the 22 attackers show that 7 (31.8%) were between 30 and 40 years old. In relation to color, 14 (63.6%) were white and had complete or incomplete primary education. Information regarding the remuneration was not included in 10 (45.5%) police reports. It was noticed that a significant proportion of offenders (27%) used of licit and/or illicit.
TABLE 3:
Distribution of cases of sexual violence according to the profile of the
perpetrators. Rio Grande/RS, 2012. (N=22)
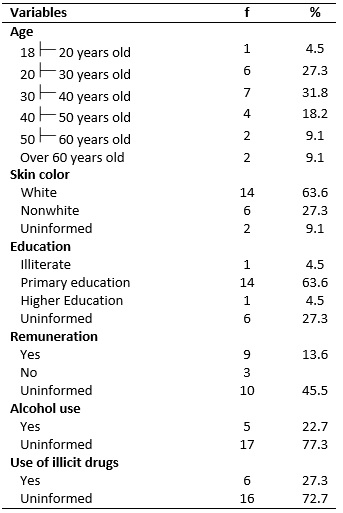
Analyzing the profile of the attackers it was observed that they had less education than the victims. Most were white, aged between 20 and 40 years and had complete or incomplete primary education, resembling the findings of other studies26. None had high school and one was a dentist. According to the literature, most offenders have low level of education26.
In addition to the macho culture that has legitimized the domain of men over women, there are different factors that trigger violent acts, including drug use, social vulnerability, intergenerational violence 1. Police reports revealed the use of alcohol and illicit drugs by the perpetrator. It is known that the use of these substances weakens the individual's inhibitions and can contribute to the manifestation of violence. Some men use this device as an excuse for violent behavior27.
These triggering factors do not justify violence against women, but become relevant as the identification thereof allows preventing these attacks. This highlights the importance of correct and complete filling of police reports as a way to contribute to the characterization of the perpetrators, victims and the dynamics of violence against women.
CONCLUSION
The study depicts the characterization of sexual violence complaints carried out in a specialized police station as well as aspects of forensic examination. By analyzing the time elapsed between sexual violence and denunciation of the aggressor, it was found a period ranging from a few hours up to 1 year and 2 months. Most of the perpetrators were strangers. The lack of bond seems to be a facilitator to the complaint, for women who have been raped by an intimate partner, family members and acquaintances took longer to register the complaint.
Similarly, women who had given up their complaint against the perpetrator were victimized by men close to them. The forensic examination, achieved for proving the fact, for identification and criminalization of the perpetrator, was often conducted by a physician.
The profile of the victims who underwent forensic examination was of white young women with complete or incomplete high school. Offenders were generally older and had less education than the victims. The police reports registered use of alcohol and other drugs by the perpetrator. As study limitation we highlight the lack of complete filling of the information contained in police reports, which hinders or impedes the correct view of the problem. Such data are essential for the design and implementation of actions aimed at addressing and preventing sexual violence.
In addition, this study highlights the need for intersectoral and humanized care to victims from the time of the complaint, so that the consequences of this aggression are minimized, until the collection of evidence to prevent impunity for perpetrators.
REFERENCES
1. World Health Organization. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence [Internet]. 2013. [cited in Apr 10 2016]. Available in: http://apps.who.int/iris/bitstream/10665/85239/1/9789241564625_eng.pdf?ua=1
2. Diniz NMF, Almeida LCG, Ribeiro BCS, Macêdo VG. Female victims of sexual violence: adherence to HIV chemoprophylaxis. Rev Latino-Am Enfermagem. 2007; 15: 7-12.
3. Núñez A, Tortolero Y, Verschuur A, Camacaro M, Mendoza S. Sexual violence. A hidden phenomenon in legal and forensic expertise. Rev Obstet Ginecol Venez. 2008; 68: 233-39.
4. Almeida LR, Silva ATMC, Machado LS. The object, the purpose and the instruments of healthcare work processes in attending to gender-based violence in a primary care service. Interface – Comunic, Saude, Educ. 2014; 18: 47-59.
5. Gomes NP, Bomfim ANA, Diniz NMF, Souza SS, Couto TM. Perception of professionals working in the service network on combating violence against women . Rev enferm UERJ. 2012; 20:173-8.
6. Gomes NP, Bonfim ANA, Barros RD, Silva Filho CC, Diniz NMF. Facing domestic violence within the family health strategy. Rev enferm UERJ. 2014; 22:477-81
7. Brazil. Law No. 12,015 of August, 7, 2009 [Internet]. 2009. [cited in March 25, 2016]. Available in: http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2009/lei/l12015.htm
8. World Health Organization. Violence against women [Internet]. 2009. [cited in Mar 26 2016]. Available in: http://www.who.int/mediacentre/factsheets/fs239/es/
9. Cerqueira D, Coelho DSC. Rape in Brazil:. An X-ray according to the health data. Applied Economic Research Institute. Brasília: IPEA [Internet]. 2014. [cited in Mar 26 2016]. Available in: http://www.compromissoeatitude.org.br/wp-content/uploads/2014/03/IPEA_estupronobrasil_dadosdasaude_marco2014.pdf
10. Raj A, McDougal L. Sexual violence and rape in India. The Lancet [Internet]. 2014. [cited in Mar 30 2016]; 383: 865. Available in: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2814%2960435-9/fulltext
11. Ministry of Health (Br). Secretariat of Health Care. Department of Strategic Programmatic Actions. Prevention and treatment of injuries resulting from sexual violence against women and adolescents: technical standard. 3rd ed. Brasilia: Publisher of Ministry of Health; 2012.
12. Drezet J, Junqueira L, Tardelli R, Antonio IP, Macedo Jr, Vertamatti MAF et al. Influence of medical and legal examination on the accountability of the author of the sexual violence against adolescents. Rev Bras Crescimento Desenvolvimento Hum. 2011; 21: 189-97.
13. Acosta DF, Gomes VLO, Barlem ELD. Profile of police reports of violence against women. Acta Paul Enferm. 2013, 26: 547-53.
14. Leite MTS, Figueiredo MFS, Dias OV, Vieira MA, Souza LPS, Mendes DC. Occurrence of violence against women in different life cycles. Rev Latino-Am Enfermagem. 2014; 22: 1-8.
15. Gadoni-Costa LM, Zucatti APN, Dell'Aglio DD. Violence against women: survey of cases seen in the psychology department of a women's police station. Estud psicol. Campinas. 2011; 28: 219-27.
16. Facuri CO, Fernandes MAS, Oliveira KD, Andrade TS, Azevedo RCS. Sexual violence: a descriptive study of the victims and the care in a university reference service in the State of Sao Paulo, Brazil. Cad Saúde Pública. 2013, 29: 889-98.
17. Teixeira PAS, Pinto AS, Moraes OCR organizers. Women's Dossier 2013. Public Safety Institute. [Internet]. 2013. [cited in Mar 6 2016]. Available in: http://arquivos.proderj.rj.gov.br/isp_imagens/Uploads/DossieMulher2013.pdf .
18. Schraiber LB, d'Oliveira AFPL, França-Jr. I, Diniz SD, Portella AP, Ludermir AB et al. Prevalence of violence against women by an intimate partner in Brazilian regions. Rev Saude Publica. 2007; 41: 797-807.
19. Federal government. Applied Economic Research Institute. Social tolerance to violence against women. Secretariat of Strategic Issues of the Presidency [Internet]. 2014. [cited in Mar 10 2016]. Available in: http://www.ipea.gov.br/portal/images/stories/PDFs/SIPS/140327_sips_'violencia_mulheres.pdf
20. Janisch S, Meyer H, Germerott T, Schulz Y, Albrecht UV, Schmidt A et al. Analysis of clinical forensic examination reports on sexually abused children. Arch Kriminol. 2010; 225: 18-27.
21. Guimarães JATL, Villela WV. Characteristics of physical and sexual violence against children and adolescents in the MLI in Maceio, Alagoas, Brazil. Cad Saúde Pública. 2011; 27: 1647-53.
22. Ministry of Health (Br). Law No. 8862 of March 28, 1994 [Internet]. 1994. [cited in Mar 10 2016]. Available in: http://www.planalto.gov.br/ccivil_03/Leis/1989_1994/L8862.htm
23. Madi SRC, Knob LF, Lorencetti J, Marcon NO, Madi JM. Sexual violence: experience of Care Program for Victims of Sexual Violence PRAVIVIS, of the General Hospital of Caxias do Sul, RS, Brazil. Revista da AMRIGS. Porto Alegre. 2010; 54: 13-8.
24. Debert GG, Oliveira MB. The conciliatory models of conflict resolution and "domestic violence". Cadernos Pagu. 2007; 29: 305-37.
25. Okabe I, Fonseca RMGS. Violence against women: contributions and limitations of the information system. Rev esc enferm USP. 2009; 43: 453-8.
26. Griebler CN, Borges JL. Violence against women: a profile of those involved in police reports of the Maria da Penha Law. Psico. 2013; 44: 215-25.
27. Deeke LP, Boing AF, Oliveira WF, Coelho EBSC. The dynamics of domestic violence: an analysis from the speeches of the attacked woman and her partner. Saude soc. 2009; 18: 248-58.