RESEARCH ARTICLES
Provoked abortion: social representations of women
Bárbara Angélica Gómez PérezI; Nadirlene Pereira GomesII; Maria de Fátima de Souza SantosIII; Normélia Maria Freire DinizIV
IUniversity Professor from the School of Nursing at the UNIJORGE University. Salvador, Bahia, Brazil. E-mail: baby_agp@yahoo.com.br.
IIUniversity Associated Professor from the School of Nursing at the Federal University of Bahia. Salvador, Bahia, Brazil. E-mail: nadirlenegomes@hotmail.com.
IIIUniversity Associated Professor from the Department of Psychology at the Federal University of Pernambuco. Recife, Pernambuco, Brazil. E-mail: mfsantos@ufpe.br.
IVAdjunct University Professor from the School of Nursing at the Federal University of Bahia. Salvador, Bahia, Brazil. E-mail: normeliadiniz@gmail.com.
ABSTRACT
This is a study with quantitative approach, grounded on the Word Association Test. The research was aimed at capturing the content and structure of social representations of women about provoked abortion. The study subjects were 147 women who had provoked abortion, with the locus in a public maternity of the city of Salvador (BA). The Word Association Test was used, in the year 2007. The data was processed by the EVOC 2000 software. The structure of the representations is supported by the elements of the central core that qualify the act of the provoked abortion (crime and sin), motivate the practice (courage and situation of each one) and express the consequences of its accomplishment (pain, regret, guilt, death and sadness), and by the elements of the peripheral core (medication, prejudice, wickedness, weak, anger and difficult). The health care professionals might develop actions to redefine such representations, because they result in the illness of these women, and think of strategies that guarantee a judgment-free attendance (care).
Keywords: Provoked abortion; Domestic violence; Woman’s health; Nursing.
INTRODUCTION
Worldwide, approximately half a million pregnant women die every year. Of these, 13% lose their lives as a result of abortions performed in unsafe conditions, which corresponds to approximately 67 thousand annual deaths1.
Pregnancy termination is the fourth leading cause of hospitalizations in the Brazilian public health network and is the fourth leading cause of maternal death, and in the cities of the Northeast Region of the above mentioned country is one of the most significant causes. In Salvador, since the early 1990s, abortion continues to be the leading cause of death among women of childbearing age2,3.
In 2000, the number of illegal abortions in Brazil ranged between 750 thousand and 1,4 million. Nevertheless, this number corresponds only to women hospitalized in the SUS, in view that, for being illegal, there is no way to obtain actual data2. The omission of records is a worrying situation, since it fails to mention the actual values of incidence of abortions and conceals the magnitude of sequels of induced abortions. This situation can only be soothed through the decriminalization of abortion in Brazil.
Due to the fact of not having a legal character, abortion is conducted under precarious conditions of safety and hygiene, which provokes an increase in morbidity and mortality rates, especially among women with low purchasing power. Among the reasons associated with the decision to abort, one can find poverty, fear of abandonment (by the partner), family rejection and lack of job opportunities4.
The experience of violence among Brazilian women is a decisive factor for the abortion process. Women in situation of provoked abortion feel guilty for having destroyed a life; they have a fear of being judged by others for having made an abortion and suffer the discriminatory actions of some health care professionals1.
Under this perspective, we question: What are the representations that women have about provoked abortion? In order to answer this question, we have adopted the following study object: the social representations of women about provoked abortion. We tracked the aim of capturing the content and structure of social representations of women about provoked abortion.
LITERATURE REVIEW
According to the Technical Standard of Humanized Care to Abortion, it affects young women and interferes in their physical, mental and reproductive health, since it causes immediate physical complications such as hemorrhages, infections, perforations of organs and infertility, and it all is added up to the subjective aspects of scapegoat and criminalization of the abortion process1.
The Latin America and Caribbean countries are among those with the most restrictive legislations in relation to abortion. Some countries demonstrate flexibility in their laws, thereby allowing abortion in situations that offer risk to the woman’s life, such as, for example, in cases of rape and in some fetal abnormalities. In some countries, such as Cuba, Barbados, Puerto Rico and, more recently, in Guyana, abortion might be performed in any circumstances at the request of the woman, without considering this act as a crime2.
In the Brazilian Criminal Code of 1940, abortion is ranked among the crimes against life, and is considered a crime. Nonetheless, abortion is only legally supported by the Article 128, which authorizes abortion practiced by a physician in cases of risk of life for the pregnant woman or when the pregnancy results from rape, in which case there must be consent on the part of the pregnant woman or her legal representative, when she is unable. Nevertheless, only from the 1980s, the first attendances in the Brazilian public health service were officially performed4.
Although the Brazilian Criminal Code provides for legal abortion for more than 50 years, one can observe a political disorganization on the part of governments and the public health system, which affects sexual and reproductive rights of women.
Research reveals that many health care professionals disregard the social questions that stem from the issue of clandestinity of abortion and also the sexual and reproductive rights of women, thereby limiting the perception of abortion as criminal practice.
The various statements of the Pope and representatives of the Catholic Church, with regard to abortion, are based on teachings that address abortion as a crime against life. Accordingly, religion has great influence on the ideas that women have about sin, guilt and fear, even among those who did not provoke abortion6.
Thus, the free decision on how to deal with the questions of contraception, of voluntary interruption of pregnancy, with the exercise of sexuality and the option of having children or not, is still a distant possibility for many women. Nonetheless, from the 1970s, they started to question the inequality between men and women and discuss themes such as: the right to their bodies, the sexual pleasure disconnected from procreation, the demystification of the body as an object belonging to male gender and issues of violence. All the above mentioned items have undermined women. Accordingly, the feminist movement aroused against the male supremacy7.
In the gender approach, responsibility for conception and motherhood is assigned to women8. From which one realizes that it is a task of the woman to decide about maintaining pregnancy or stopping it, so that, when deciding for abortion, she is the one responsible for this attitude. Thus, anchored in gender matters, the women’s movement has contributed to the introduction of the restrictive questions for the private gender relationships into the National Policy Agenda, such as sexuality and reproduction; contraception; prevention of sexually transmitted diseases and the fight to legalize abortion.
In order to meet these standards, it becomes necessary to create spaces for the introduction of gender matters and sexual and reproductive rights of women. A quantitative study highlights the importance of nursing in this process9.
THEORETICAL AND METHODOLOGICAL BENCHMARK
This is a quantitative study, based on the structural approach of the Social Representations Theory. The choice of the Social Representations Theory as a theoretical basis is linked to its capacity to unravel the thinking of society about an object shared in everyday life, which, in this study, will be the socially constructed knowledge and suitable in relation to abortions provoked by women.
According to the structural approach, the social representation is organized into a central system and in peripheral systems arranged around this, thereby constituting essential parts of the content of the representation, i.e., its more accessible, more alive and more complete components. Accordingly, the central core ensures meaning, consistency and persistence of the representation, which gives it the resistance to the change. In turn, the peripheral system is more flexible and protects the central core, which allows the fusion of different information and social practices, and it is fundamental to the core as it allows the anchoring of reality10.
The study was conducted in a public maternity in Salvador (BA), which is a unit of the Department of Health of the Bahia State (SESAB) that is reference in assisting women in the reproductive period. The study subjects were 147 women hospitalized because of provoked abortions, after hospital discharge.
The ethical aspects regulated by the National Health Council (CNS) were followed, according to the Resolution nº 196/96, which guides the ethics in researches with human beings. The project was approved by the Ethics Research Committee from the Health Department of the Bahia State (CEPSESAB), as the Opinion nº 20/266, Letter 36/2006.
The Word Association Test (WAT) was used as instrument for data collection, processed through the EVOC 2000 software. The WAT is a technique for the collection of elements that constitute a representation, in which one made use of stimuli, and these might be verbal or not, with the purpose of evoking implicit or latent answers in relation to the object to be investigated11.
Conducted between March and June 2007, the WAT contained an open question for the expression of the free association of words, which was related with the question: What are the words that come to your mind when I say “abortion”? The answers have allowed revealing the average frequency of the most evoked words by women and identifying the elements of the central core of social representations.
The process of organizing and analyzing basically involved the organization of words by order of frequency and average of evocation. Thus, it has allowed identifying the structure of the social representation of women in relation to abortion, by highlighting elements of the central core and the peripheral system.
The data were presented in diagrammatic form, where one can find the central core and the peripheral elements. The position of elements in quadrants is defined by frequency of occurrence. In the upper left quadrant of the diagram, there are the elements that define the central core of the representation, for presenting the highest frequency of occurrence and ready evocation. In the lower right quadrant, there are the predominant results, with less frequency and late evocation, which composes the elements of the peripheral system of the representation11.
RESULTS
The subjects are predominantly characterized for being young and black women with low schooling level; they live with a spouse, are unpaid domestic workers, economically dependent on their husbands/partners; had one or two pregnancies, deliveries and/or children, performed abortion for the first time; with the economic situation, the domestic violence, the young age and the fact of hampering plans for the future as the most reported reasons for the practice of abortion.
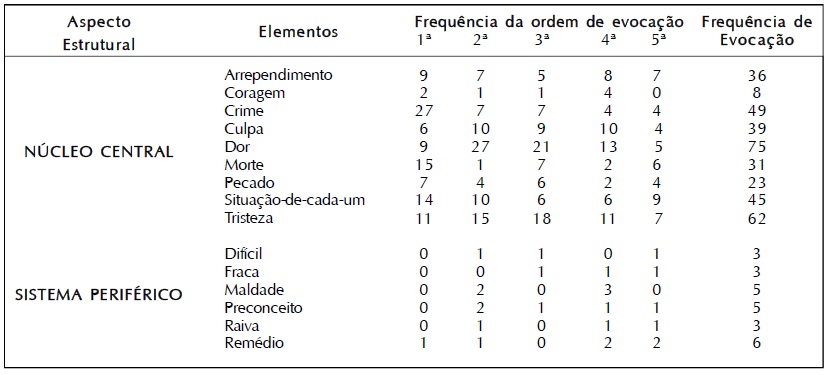
From the 147 women who answered the WAT, 732 evoked words were obtained, and, of these, only 27 different words were found, thereby demonstrating the little dispersion of senses in relation to abortion, which drives us to think that the data found in this survey are quite consensual, i.e., the social representation of abortion in this group presents itself strongly shared by women, so that the meaning of abortion is organized around few elements, as shown in Figure 1.
FIGURE 1: Average order of words of social representations of women in relation to provoked abortion. Salvador (BA), 2006.
The central core of the representation of women in relation to abortion is anchored in their experiences and in values and concepts developed about this matter, and this representation influences their behaviors. Accordingly, the words that comprise the core are: pain, sadness, crime, situation of each one, guilt, regret, death, sin and courage.
The surveyed women have considered these elements as the most important in representing the provoked abortion and they are those who give meaning to their representations. Accordingly, such items are considered consensual, stable, collectively shared and normative, and they are materialized by the elements of the peripheral system, which are organized around the central core and depict the actual situation in which the representation is elaborated or put into operation10.
The words that comprise the peripheral system are: medication, prejudice, wickedness, weak, anger and difficult. Because they are more flexible and, therefore, show less resistance to changes, enable individual modulations that allow flexibility and elasticity in the elaboration of social representations. The peripheral system, regarding its functionality, represents the position-taking or behavior, referring to the study object.
DISCUSSION
The study showed that crime and sin emerged as the elements of the central core that qualify the act of provoked abortion, since they are anchored in the religious and moral values of our society, given that, in Brazil, provoked abortion is considered a criminal practice.
The sin has strong legal and religious influence for women, because they feel that they have transgressed the human being’s law and also the God’s law. Religious influences are always present in discussions about abortion in Brazil, although the country is considered a Secular State. Abortion appears as a sin against life, a murder, something despicable, which conveys the idea that the religious precepts are unquestionable. In Christianity, the question of abortion is seen as an abominable sin among religious people, and is considered a serious crime against life, and deplorable, since, when practicing an abortion, the woman should renounce her religious creed12.
In this sense, women, when opting to perform clandestine abortions, are seen as criminals who, individually, decided to commit an offense. Thus, when reaching the health care services, women omit the reality of the process of provoked abortion, thereby reporting only physical complaints. Research emphasizes that, when a woman provokes abortion, only seeks a health care service when she has complications, because, in most cases, is treated as guilty and criminal by the professionals who attend this type of occurrence. Therefore, the assistance is guided by the idea that abortion is a criminal act, without considering the reproductive rights or the social questions of women.
Even knowing the risks and the suffering that they might face, women provoke abortion, driven by the courage to face all the problems involved in its accomplishment. The pregnancy termination is presented and justified by women by means of: economic situation, domestic violence, young age, not being prepared, other plans for the future and lack of a partner12.
From this perspective, being faced with an unwanted pregnancy is a possibility for every woman of childbearing age with active sexual life, even those who use contraceptives in a correct manner, given the non-existence of a method that ensures the total absence of pregnancy, i.e., in spite of the care actions, unwanted pregnancy is part of women’s lives. Hence, this is the female dilemma: should I stay with the child, fruit of an unwanted pregnancy, or provoke abortion? None of these alternatives would be an exit exempt from suffering for women who find themselves alone, when having to choose between two solutions, neither of which is satisfactory, and in a solitary way, they, finally, take a decision.
When deciding to perform a provoked abortion, women start to experience different feelings: pain, regret, guilt, death, sadness, among others. For the majority of women, the abortion process is painful and uncomfortable, and emotional factors might influence in the perception of pain. Thus, it becomes necessary to have attention on the part of health care professionals for controlling and relieving pain. With regard to pain, the inappropriate care of women causes unnecessary suffering and might increase anxiety and generate complications1.
The pain is a symptom that denotes that the abortion process was triggered, so that the woman already knows that when using Cytotec (Misoprostol). Another aspect that contributes to the pain is the clandestinity. In this condition, women keep their suffering in silence or, at most, share it with people of their trust, since they have a fear of the judgment of the other and do not find support, even in health care services8. The emotional pain is closely related with provoked abortion, since the woman is the one who decides who ingests and introduces the medication, which, for the majority, is an experience of deep suffering and sadness.
Women associate the regret with a diversity of feelings arising from painful experiences, but, for some of them, abortion was necessary at that time, often, the unique option. Study also mentions that some women develop, after abortion, emotional reactions coming from guilt, such as remorse, regret and sense of loss, uncomfortable feelings for them, including being a relevant risk factor for depression13.
Many of the interviewees feel guilty even before performing an abortion, which is strengthened by social, cultural and religious values that permeate the social representations. The abortion process is loaded with much suffering, because of the feelings that the women experience and that are enhanced when they are faced with the gaze of prejudice of the other, since there is a stigma before the provoked abortion14.
Feelings of guilt, remorse and shame are manifestations resulting from social standards. The shy about talking about abortion is nothing more than the fear of being exposed and humiliated. For the Freudian Psychoanalysis, the feeling of guilt corresponds to an internal conflict that results in self-punishment, of remorse that results from the perception of the individual by violating moral rules, for the welfare of others15.
Women already know that abortion might lead to death, knowledge transmitted by women who tell histories of others who have died, by media and by health care professionals. The Brazilian Ministry of Health recognizes through the Technical Standard of Humanized Care to Abortion that miscarriage performed in unsafe conditions is a major cause of maternal death, and the late care to an unsafe abortion and its complications might threaten the physical and mental health of a woman, as well as her own life1. However, this standard has not been able to guarantee changes in attendance, as we can realize that women continue to die as a consequence of unsafe abortions and the prejudice on the part of health care professionals, permeated by the stigma, still remains.
In this sense, we realize that, for women, death is actual, experienced in a very painful manner, brought by fear. It is the expression of a deepest anguish, the vital anguish13. Then, we can see that women, when experiencing the process of provoked abortion, experience a great sadness, together with the ambiguity of wanting and not wanting to provoke cases of abortion and, at the same time, consider the solitary practice of provoked abortion as the unique solution. This ambiguity, in turn, translates another feeling: the guilt. From the legal and religious viewpoint, the guilt is inserted in the context of criminality.
However, the provoked abortion permeates the attitudes of women, which involves the ideas that each one has in relation to the theme, her manner of being and her experiences, thereby influencing the practice at stake.
We can observe that medications act as an exit for the success of the practice of provoked abortion and establishes an interface with the elements of the central core “pain and death”, because, when using the drug (Cytotec), the woman already know that will feel pain. She also knows the risk of death inherent to the unsafe practice of the provoked abortion. Accordingly, the use of Cytotec medication is a knowledge acquired by women and a practice used by them for causing miscarriage, and is also one of the techniques of choice for elective abortion provided in law, which are recommended by the Brazilian Ministry of Health1,16.
Regarding the words “prejudice” and “wickedness”, they establish an interface with the elements “crime”, “guilt” and “sin”, represented in the central core, because the moral, legal and religious questions are intertwined in the representation of provoked abortion, thereby reinforcing these feelings. The words “difficult” and “weak”, belonging to the peripheral system, are associated with the pain and the courage of the woman, because she is the one who experiences, alone, the decision to ingest and introduce the medication. The word “anger”, belonging to the peripheral system, is associated with the term “situation” of each one of the central core, given that many of them relate anger with situations of domestic violence that end up influencing in their decision for abortion. Therefore, we can realize that the peripheral system provides an interface to the central core, which results in the construction of the representation of provoked abortion, since both express objective and subjective elements. This shows that the social representation feeds both on scientific theories and on culture, ideologies and experiences.
Research also developed in Salvador (BA) corroborates the complexity around the woman’s decision for inducing the abortion process. The economic constraints, the experience of violence in the marital relationship and the fear of losing her autonomy were mentioned as reasons related to the decision17. In light of the above mentioned context, abortion is often revealed as the unique solution. Whatever the choice - having the child or aborting, women will have to deal with situations that will change their lives17,18.
The study conducted in Salvador (BA) also showed that, from the first moment in which they find themselves pregnant, the women hospitalized in public maternities experience a painful process, permeated by feelings of guilt and anguish17. Whereas such experience undermines women for physical and mental illness, it is argued a listen and welcoming of professionals that allow women to express their feelings and, consequently, offer a better health care for those who decide for abortion17. It is worth highlighting that the professional behavior in relation to the woman in the abortion process must not be subjected to the individual conscience, which is grounded on moral values, but on the behaviors designed and established in codes of ethics that orient the professional action. In this sense, it should be remembered that a health care with quality is an ethical prerogative in caring for people, and it must be a priority at the time of attendance.
It is from the human comprehension that we learn to recognize the other as subject and, thereby, enhance the aspects related with the intersubjectivity of the provoked abortion, and it is imperative to integrate professionals from various fields of study that allow themselves to acquire an comprehension permeated by openness, generosity and solidarity.
Under this perspective, the scholars of this theme and/or the professionals who assist women in situations of provoked abortion, need to comprehend abortion as a public health problem, and must not be restricted to technical aspects of care to women, but creating conditions for combating dehumanization, especially when it is a still very stigmatized situation, so that these women are respected as citizens.
CONCLUSION
In order to comprehend the representations of women about the provoked abortion, the study showed that its structure is sustained by the elements of the central core that qualify the act of the provoked abortion (crime and sin), motivate the practice of such act (courage and situation of each one) and express the consequences of the accomplishment of an abortion (pain, regret, guilt, death and sadness), and by the elements of the peripheral core (medication, prejudice, wickedness, weak, anger and difficult), which are organized around the central core. It is worth emphasizing that, because they are more weakly anchored in standards, values and beliefs, the elements of peripheral cores are less resistant to changes and, therefore, considered more easily vulnerable to transformations.
The absorption of social representation shared by women who provoke abortion is essential in the sense of favoring the comprehension, on the part of health care professionals, of the complexity around the abortion-related decision and the act of abortion. The comprehensive gaze towards women in situations of abortion might unveil lives permeated by pain, by sadness and by guilt, especially because they consider themselves as criminals. The work of professionals must not reinforce such representation. Accordingly, it becomes necessary to deal with representations, because they result in the illness of these women.
This study is limited by the uniqueness of the group of surveyed women. Nonetheless, although the social representations in relation to abortion have been absorbed by women living in a city with cultural, religious and social quirks and specificities, it is crucial to think about strategies that enhance the trust between health care professionals and women. In the field of health education, health care professionals, especially those who work in spaces of family planning, whether in maternities or in the scope of the Family Health Strategy (FHS), might develop actions to redefine such representations, anchored on the stigma that permeates the abortion, in order to help them to minimize/ repeal such suffering.
REFERENCES
1. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Área Técnica de Saúde da Mulher. Atenção humanizada ao abortamento: norma técnica. Brasília (DF): Ministério da Saúde; 2005.
2. Ministério da Saúde (Br). Portal da Saúde (SUS). Aborto inseguro: um problema de saúde pública. Norma técnica humaniza atendimento às mulheres com complicações de abortamento. 2011. [citado em 05 mai 2013]. Available at: http://portal.saude.gov.br/saude/visualizar_texto.cfm?idtxt=22411.
3. Nery IS, Monteiro CFS, Luz MHBA, Crizóstomo CD. Vivências de mulheres em situação de aborto espontâneo. Rev enferm UERJ. 2006; 14:67-73.
4. Soares GS. Toques de saúde aborto. João Pessoa (PB): Cunha Coletivo Feminista; 2004.
5. Sandi S, Braz M. As mulheres brasileiras e o aborto: uma abordagem bioética na saúde pública. Revista Bioética. 2010; 18(1): 35-51.
6. Pereira IG, Rosado-Nunes MJ, Jurkewicz RS, Pimentel S, Pandjiarjian V, Frigério V, et al. Aborto legal: implicações éticas e religiosas. São Paulo (SP): CDD; 2002.
7. Souza ZCSN, Diniz NMF. Aborto provocado: o discurso das mulheres sobre suas relações familiares. Texto contexto - enferm. 2011; 20:742-50.
8. Pérez BAG. Aborto provocado: representações sociais de mulheres [dissertação de mestrado]. Salvador (BA): Universidade Federal da Bahia, 2006.
9. Martins CBG, Alencastro LCS, Mato KF, Almeida FM, Souza SPS, Nascimento SCF. As questões de gênero quanto à sexualidade dos adolescentes. Rev enferm UERJ. 2012; 20:98-104.
10. Abric JC. A abordagem estrutural das representações sociais: desenvolvimentos recentes. In: Campos PHF, Loureiro MCS, organizadores. Representações sociais e práticas educativas. Goiânia (GO): UCG; 2003. p. 37-57.
11. Sá CP. Núcleo central das representações sociais. Rio de Janeiro: Vozes; 1996.
12. Paucar LMO. Representação da gravidez e aborto na adolescência: estudo de casos em São Luís do Maranhão [dissertação mestrado]. Campinas: Universidade Estadual de Campinas; 2003.
13. Benute GRG, Nomura RMY, Pereira PP, Lúcia MCS, Zugaib M. Abortamento espontâneo e provocado: ansiedade, depressão e culpa. Rev Asso Med Bras. 2009; 55(3):322-7.
14. Leitão HAL. Diferenças sexuais no desenvolvimento da preocupação moral por outras pessoas: um estudo empírico da expressão de emoções morais em crianças. Psicol Reflex Crit. 1999; 12(1):21-46.
15. Ballone GJ. PsiqWeb Psiquiatria Geral [site de Internet]. Medos, fobias & outros bichos. [citado em 21 jun 2005] Available at: http://gballone.sites.uol.com.br/voce/medos.html.
16. Gesteira SMA. Assistência prestada à mulher em processo de aborto provocado: o discurso das mulheres [tese doutorado]. São Paulo: Universidade Federal de São Paulo; 2006.
17. Pereira VN, Oliveira FA, Gomes NP, Couto TM, Paixão GPN. Abortamento induzido: vivência de mulheres baianas. Saude soc. 2012; 21:1056-62.
18. Pacagnella RC. Novamente a questão do aborto no Brasil: ventos de mudança?. Rev Bras Ginecol Obstet. 2013; 35(1):1-4.
Recebido em: 05.11.2012
Aprovado em: 06.10.2013