(*) Videos uploaded on the YouTube site before February 27, 2014.
ORIGINAL RESEARCH
Men's participation during childbirth: Youtube videos
Isaiane da Silva CarvalhoI; Camila Fernandes da Silva CarvalhoII; Bertha Cruz EndersIII; Rosineide Santana de Brito IV
I
Nurse. Master's degree in nursing. Ph.D. student in nursing, Federal
University of Rio Grande do Norte. Brazil. E-mail:
isaianekarvalho@hotmail.com
II
Nurse. Master's degree in nursing, Federal University of Rio Grande do
Norte. Brazil. E-mail: camilafscarvalho@gmail.com
III
Nurse. Ph.D. in nursing. Collaborating professor, Federal University of Rio
Grande do Norte. Brazil. E-mail: bertha@ufrnet.br
IV
Nurse. Ph.D. in nursing. Associate professor, Federal University of Rio
Grande do Norte. Brazil. E-mail: rosineide@ufrnet.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.11474
ABSTRACT
Objective: to analyze videos shared on the YouTube social network relating to the man's role in childbirth. Method: in this quantitative descriptive study, selection of material on the Youtube website occurred in a single data collection session on February 27, 2014, which resulted in a sample of 40 videos. Results: fathers' participation was significantly associated with the type of filming (p = 0.004), year posted (p = 0.034), place of birth (p = 0.000), and type of delivery (p = 0.000). Among hospital births, men were recorded participating passively in 29 (85.3%) videos, and in cesarean sections, in 23 (95.8%). Conclusion: it is necessary for labor and birth to be more widely humanized in order to assure couple's rights in full, and guarantee that this moment is a pleasurable experience.
Keywords: Obstetrical nursing; paternity; parturition; webcasts.
INTRODUCTION
The importance of the presence of the partner during labor and delivery has been recognized with recommendations of the World Health Organization 1 and documented by scientific publications. Studies show that the accompaniment of the male partner and his active participation in the event, promote emotional support to the woman and facilitate his transition to the father role 2,3. However, there are still difficulties and resistance of health services in inserting the partner within the childbirth setting. When there is agreement to their participation, there is no adequate preparation for the birth experience and thus conflicting feelings may interfere in the man's actions during the labor of his partner 4.
One of the main reasons for the success of the man's participation is by educating the population. This, when conveyed in the mass media, tends to result in a positive balance, because after the development of information technology, several social networking services have become available on the internet, including YouTube - a free and open video display platform. A study developed with videos related to a particular treatment for multiple sclerosis found YouTube to be a tool that supported the struggles of the particular social group in focus. Furthermore, the publication of audiovisual records in YouTube allows an exchange of experiences and, consequently, more interest in the topic addressed, thereby proving the strength of this medium 5. This reality can be interpreted in different ways, and can be conceived as favorable or unfavorable in the context experienced by the person watching the video. This is also observed in the experience of the childbirth process, in which the participants of this moment sometimes register and publicize their experience on this social network.
In view of the above, the current study aimed to analyze videos shared in the YouTube social network regarding the forms of participation of the man accompanying a woman at the birth of a child. It should be stressed that there is little research in respect to the participation of men during childbirth using audiovisual resources. Hence, when acting as an information disseminator, YouTube has a significant relevance in the guiding of opinions, making it a favorable place for the investigation of the object of study.
LITERATURE REVIEW
At the beginning of the 20th century, the childbirth process was considered exclusively female, but with the progress of the medical sciences, this event entered the technocratic hospital space. The woman has become passive and alone in a hostile and unfamiliar environment. This scenario is gradually changing with the humanization of childbirth, which includes the importance of a companion during the entire pregnancy-puerperal cycle 6. This incentive is based on the recommendations of the World Health Organization in 19961 and in Brazil by Law No. 11.108 of April 7, 20057 which guarantees the women's right to have a companion of their choice.
In spite of this, the presence of this new person during childbirth causes difficulties, especially when it is the mother's partner, due to ignorance of his rights as a father. Additionally, other obstacles are encountered in particular barriers imposed by the institution, by the culture and by the man himself and his family8. Moreover, health professionals, divided as to the real role of the father during the birth of his child, adopt contradictory attitudes towards this situation9.
Although the difficulties in bringing the man to the delivery room are evident, studies show a gradual change in the childbirth process due, in particular, to the integration of the family as evidenced by the institutions' attempts to encourage a more active participation of the partner with physical and/or emotional support of the pregnant woman 10,11. It is also pointed out that the presence of the father contributes to a reduction in the painful experiences and suffering, sometimes experienced by women during delivery, as well as preventing unnecessary procedures12,13. Hence, starting in the prenatal period, the participation of the man is important in order for him to understand the pregnancy-puerperal cycle and his role in the whole process, thus initiating his transition to fatherhood13. However, these changes occur at a slow pace and many passive or even absent actions of man prevail in this setting.
METHODS
This is a descriptive and quantitative research developed from an analysis of videos related to the participation of men during the birth of their children found in the YouTube site (http://www.youtube.com/). The site, which was founded in 2005, was selected because it is the main video-sharing platform on the Internet and is accessed by billions of people14. The selection of the material occurred in a short data collection period on February 27, 2014. In order to do this, we used the following health sciences descriptors (DeCS) 'Parent' and 'Child', used in conjunction and with quotation marks, as a means of restricting the search to videos that had both descriptors. Twenty records were presented on each search page. Only the first ten pages of results were considered, since, based on another study, users do not generally look at more than ten pages 15. The filter of the number of views (provided the site) was used as a way of classifying the videos on the first page.
Regarding the inclusion criterion, videos were considered when the father was present as companion at childbirth. Duplicates, videos divided into more than one part and those with poor image quality that might interfere with the evaluation process were excluded. Data collection was performed in pairs, independently, using a specific data collection form, which gathered information regarding the following general characteristics: type of filming (amateur/professional), title, category; date of uploading, duration, number of views, number of comments and evaluation (liked/disliked). Moreover, specific characteristics were assessed such as place of birth, type of delivery (vaginal/cesarean/forceps), positioning on the subject (favorable/unfavorable), parent's participation (active/passive), form of active participation and form of passive participation.
The initial search resulted in 200 videos. After pre-selection in respect to the title, application of the inclusion criteria, visualization of the content and the consensus among the researchers about the number of audiovisual records selected, a sample of 40 videos was obtained.
Data analysis was performed using a statistical package. Quantitative variables were expressed as means of absolute and relative frequencies, mean, minimum, maximum and standard deviation (SD) and the qualitative variables, after the categorization process, by means of absolute and relative frequencies. Fisher's exact test was used to analyze associations related to the type of filming, year of uploading, place of birth, type of delivery and type of participation. The Mann-Whitney test for independent samples was used to compare the duration of the video, number of views, comments and the likes/dislikes of the video with the type of participation. Variables with p-values <0.05 were considered statistically significant.
RESULTS AND DISCUSSION
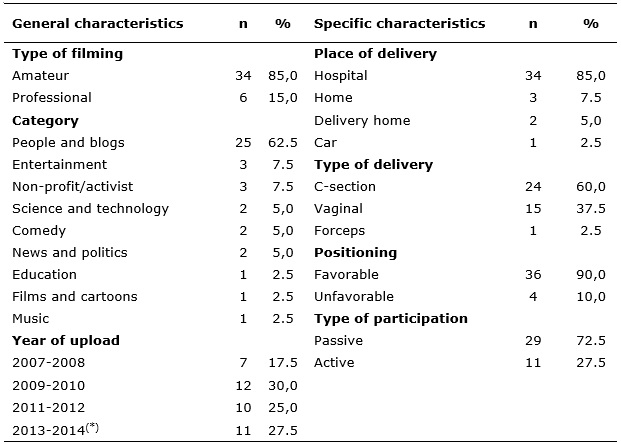
In the analysis of the 40 videos, 34 (85%) were filmed by amateurs, 25 (62.5%) were classified in the category of people and blogs and 12 (30%) were uploaded in 2009 and 2010 (Table 1). It is noteworthy that by February 27, 2014, the date of data collection, 11 (27.5%) videos had already been uploaded the period from 2013 to 2014.
Table 1:
Distribution of YouTube videos analyzed according to their general and
specific characteristics. Natal, Brazil (n = 40)
(*) Videos uploaded on the YouTube site before February 27, 2014.
The large number of amateur videos reflects a common practice of fathers during the birth of their children, at which time they act only as spectators, taking on the responsibility for recording the event themselves. A study on the father's involvement as the companion of the mother during childbirth identified that although some did not perform expected activities such as providing physical support but remained silent observing the activities occurring around them, they considered the experience of being present at that moment was very important. This fact demonstrated that they had no predefined role during the childbirth process 2.
Another study on father participation in this event reported that there are three types of actions associated with the accompanying parent. These actions were passive presence - fathers present during delivery who had no active involvement in the process; family reference – the men are available to help their partner but need guidance on what should be done; and active companion – partners who have abilities to accompany the delivery by spontaneously offering physical and emotional support 16. In general, regardless of the role played by the father, it is necessary to take into account the need to respect the peculiarities inherent in this new character, who, in the past, was excluded from the childbirth process but now is beginning to be inserted in an environment largely conceived as part of the female universe.
The growing number of videos observed in recent years is due, in particular, to changes in gender roles within society. The image of the domineering, inseminating, insensitive man gives way to a new being who is able to become emotionally involved, and willing to take responsibility, along with his partner, to care for their children. So together, man and woman experience the fascinating metamorphosis of becoming father and mother4:380. However, in spite of developments, male participation at the time of delivery is seen as being permeated by a series of obstacles such as institutional aspects and the organization of obstetrical care focused on women and children. These characteristics do not favor the legitimate right of the man to participate in the birth of his child with all the symbolism associated with that moment in the couple's life17.
The videos lasted from 29 to 1,836 seconds with an average of 382.18 seconds (SD = 349.89). The number of views varied between 19 and 573,030 with an average of 72,869.63 (SD = 156.3233,60). The frequencies of comments associated with filming ranged from 0 to 344 with a mean of 31.83 critical video observations (SD = 76.97). Regarding whether the video was liked or not, the viewers presented the following opinion: 'likes' of the video ranged from 0 to 840 with an average of 87.38 (SD = 204.37); in turn 'dislikes' varied from 0 to 60 with a mean of 5.78 (SD = 13.93). Given the data found, the high level of coverage of the videos present on YouTube is evident, especially the number of views, and thus this media is capable of influencing thousands of people, in a positive or negative way depending on the manner information is conveyed. In addition, the numbers of comments was disproportional to the number of views demonstrating that there is a tendency of not expressing opinions about the material watched and whether or not the viewer liked it.
Regarding characteristics related to childbirth, 34 (85%) occurred in hospital, 24 (60%) were C-sections, the father had a favorable position during the delivery in 36 (90%) and the father's participation was passive in 29 (72.5% %) in particular because he was responsible for filming the birth. In cases in which it was possible to identify an active participation of the father, it mostly involved (11 videos - 27.5%) providing physical and emotional support (Table 1).
The findings in respect to the place of birth are consistent with the reality in the world and in Brazil. In the United States in 2011, only 1.26% of births were performed in out-of-hospital settings,18 while in Brazil this rate reached 1.9% in the same year19. The frank growth in the incidence of C-section births around the world and the varying rates in different countries are conspicuous. This varies depending on the care model adopted, and the level of interference and participation of the State in healthcare, as well as national priorities in public health. In addition, socioeconomic and educational conditions of the population and women's choice should be taken into account; the latter is often influenced by a previous C-section, the fear of pain during labor and negative experiences of a previous normal birth20,21. Brazil is first place in the ranking of C-sections, especially elective ones, a fact corroborated by the findings of this study20. The latest data from the Brazilian Live Birth Information System for 2011 registered 1,565,564 (53.7%) C-sections compared to 1,340,324 (46.0%) vaginal deliveries19.
There are still discussions about the benefits and harm of C-sections in low-risk pregnancies. Moreover, there is no consensus on an ideal rate of C-sections consistent with the aforementioned social factors that vary across regions20. Thus, the World Health Organization recommends that a threshold limit of 10 to 15% is an acceptable cesarean rate 22.
Current attempts to return to childbirth at home or in institutions with the creation of a more pleasant environment for deliveries have been increasing in Brazil; these situations were shown in 7.5% and 5% of the videos, respectively. In these places, professional filming was made by activists or groups, who seek to spread and encourage humanized and/or natural delivery.
There was a statistically significant association between the type of the father's participation and the type of filming (p-value = 0.004), year of uploading (p-value = 0.034), place of birth (p-value = 0.000) and type of delivery (p-value = 0.000). The passive participation of the man was recorded in 29 (85.3%) videos of hospital births. There was a prevalence of passive participation in 23 (95.8%) of the C-section deliveries (Table 2).
Table 2:
Association of the general and specific characteristics of YouTube videos
with the type of paternal involvement. Natal, Brazil (n = 40)
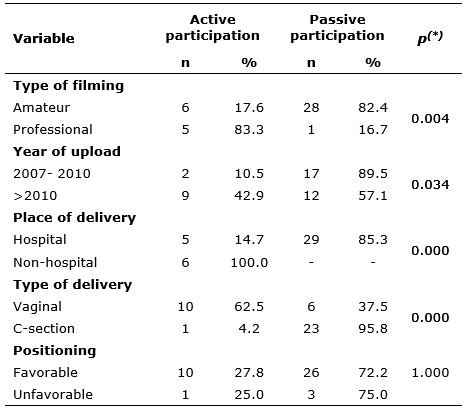
(*) Fisher's exact test
It is evident from the findings of this study that the childbirth process in a hospital environment and C-section surgery in particular are directly associated with a passive involvement of the man.
There are several reasons that may lead the father to want to participate in the birth of his child, such as his partner's request or even curiosity about this event that is so unusual within the male universe. In the same way, the experiences of these men are also different, sometimes positive and sometimes negative, ranging from a sensation of being able to offer the necessary support to the partner to the discomfort generated by the ignorance of the physiology of childbirth and the procedures performed in the delivery room23.
Thus, despite changes in relationships within the family and in the roles played by men and women, paternal participation in the pregnancy-puerperal context is still permeated by prejudices starting within the family itself. Added to this is the lack of incentive from health professionals and an obstetrical model capable of transforming a physiological event that originally occurred at home into a surgical intervention carried out in a hospital setting with the physician being the protagonist of the scene. In this context, the father is sometimes considered a stranger in the delivery room, someone to inspect the actions performed and thus, by disregarding all the benefits associated with his presence, the man is left out of the childbirth process24.
Regarding the type of delivery, it was identified that the experience of the fathers in respect to surgical delivery tends to be less pleasant compared to vaginal deliveries. A study of 20 men who experienced this moment in Blantyre, a city in southern Malawi, reported the great discomfort they presented on seeing the abdominal incision, calling the experience scary. Of the four men who watched C-sections, all stated that they had no interest in participating in a future delivery. On the other hand, the expectant fathers of vaginal deliveries were willing to experience this experience again 23. This is corroborated in the current study, in which three videos recorded the fainting of parents during childbirth with this fact being portrayed comically. Furthermore, a video simulating a delivery shows a violent father when faced with the doctor's behavior of spanking the newborn to promote crying, which is another way to criticize the moment.
Contrary to the reality of C-sections in hospital, home delivery is intrinsically related to an active participation of the man. This environment is conceived as a place conducive to the salvage of humanized childbirth, in which the woman retakes the role of protagonist and the control of her body. The presence of the man, in turn, is understood as something natural and he is constantly stimulated to participate actively at all times. In addition, professionals working in home births perceive the father/companion not as a stranger to that environment but as someone who positively favors the physiology of childbirth, with a focus on humanized care based on respect for those involved25.
It is in this context that the figure of the obstetrical nurse is a strategic agent to improve care models of childbirth guided by humanization. The practice is based on scientific evidence, which tends to find positive results with the stimulation of normal delivery 26,27. It should be emphasized, therefore, that regardless of the environment in which childbirth occurs, the birth route and the professionals involved, it is necessary to ensure humanized care, considering the yearnings and desires of women and men, giving them all the necessary support, with special attention to the integration of the father in the childbirth procedure.
Statistical analysis showed no significant association between the type of involvement of the father and the duration of the video (p-value = 0.683), the number of views (p-value = 0.988), the number of comments (p-value = 0.938) and the fact that the video is liked (p-value = 0.784). However, the number of views was higher with the passive participation of the father (mean = 91,519 views) compared to active participation (mean = 23,704 views) (Table 3).
Table 3:
Association of mean values of general characteristics of YouTube videos
with the type of paternal involvement. Natal, Brazil (n = 40)
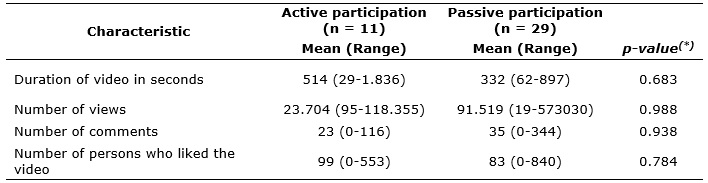
(*)
Mann-Whitney Test
This finding corroborates a research that portrayed the existence of difficulties of health professionals in understanding and articulating the role of the father in the interim of delivery, especially during C-sections 11. Thus, the number of videos showing the passivity of the father is a vehicle capable of contributing to the diffusion of this behavior.
CONCLUSION
Based on these results, the passive participation of the father during the birth of his child is evident, that is, the father is not involved in the delivery process, abstaining from physical or emotional support of his partner, even though his presence is accepted in part by the health team. This situation is reinforced when the man experiences the childbirth in the hospital particularly in a surgical environment, which are permeated as much by routines as by procedures, thereby limiting his space to participate. These restrictions were translated when the fathers, for the most part, acted as mere spectators by filming the birth.
We also stress the idea transmitted by the videos that, despite advances, the man has not yet been effectively integrated in the pregnancy-puerperal context. Thus, it is still necessary to spread the humanization of childbirth, especially among health professionals, to ensure the full rights of the couple and the preparation of both for this event starting in the prenatal period, for the childbirth process to be a pleasurable experience.
The main limitations related to the present study correspond to the fact that surveys that involve the use of social media, such as YouTube, do not have protocols that guide its methodological development. Thus, given the difficulty in finding scientific productions about the theme, new research that seeks to evaluate the impact of these videos on the viewers is suggested.
REFERENCES
1.World Health Organization. Care in normal birth: a practical guide. Genebra(Swi): WHO; 1996.
2.Perdomini FRI, Bonilha ALL. A participação do pai como acompanhante da mulher no parto. Texto & Contexto Enferm. 2011; 20(3):445-52.
3.Palinski JR, Souza SRRK, Silveira JTP, Salim NR, Gualda DMR. Women's perception on the process of coaching labor. Online Braz J Nurs. 2012; 11(2):274-88.
4.Jardim DMB, Penna CMM. Pai-acompanhante e sua compreensão sobre o processo de nascimento do filho. Rev Min Enferm. 2012; 16(3):373-81.
5.Mazanderani F, O'Neill B, Powell J. People power or pester power? YouTube as a forum for the generation of evidence and patient advocacy. Patient Educ Couns. 2013; 93(3):420-5.
6.Rattner D. Humanizing childbirth care: a brief theoretical framework. Interface Comun Saúde Educ. 2009; 13(Suppl 1):595-602.
7.Ministério da Saúde (Br). Lei nº 11.108, de 07 de abril de 2005. Altera a Lei nº 8.080, de 19 de setembro de 1990, para garantir às parturientes o direito à presença de acompanhante durante o trabalho de parto, parto e pós-parto imediato, no âmbito do Sistema Único de Saúde. Brasília (DF):Senado Federal; 2005.
8.Abushaikha L, Massah R. Perceptions of barriers to paternal presence and contribution during childbirth: an exploratory study from Syria. Birth. 2013; 40(1):61-6.
9.Carvalho IS, Júnior PBC, Macedo JBPO, Araújo RDT. Acompanhantes no processo de nascimento: benefícios reconhecidos pelos enfermeiros. J Health Sci Inst. 2013; 31(2):166-71.
10.Staudt ACP, Wagner A. Paternidade em tempos de mudança. Psicol Teor Prát. 2008; 10(1):174-85.
11.Longo CSM, Andraus LMS, Barbosa MA. Participação do acompanhante na humanização do parto e sua relação com a equipe de saúde. Rev Eletrônica Enferm. 2010; 12(2):386-91.
12.Silva RM, Barros NF, Jorge HMF, Melo LPT, Ferreira Junior AR. Evidências qualitativas sobre o acompanhamento por doulas no trabalho de parto e no parto. Ciênc Saúde Coletiva. 2012; 17(10):2783-94.
13.Oliveira ASS, Rodrigues DP, Guedes MVC, Felipe GF, Galiza FT, Monteiro LC. O acompanhante no momento do trabalho de parto e parto: percepção de puérperas. Cogitare Enferm. 2011; 16(2):247-53.
14.YouTube. YouTube [Internet]. [cited on Jan 10, 2016]. Available from: https://www.youtube.com/?hl=pt&gl=BR
15. Murugiah K, Vallakati A, Rajput K, Sood A, Challa NR. YouTube as a source of information on cardiopulmonary resuscitation. Resuscitation. 2011; 82(3):332-4.
16. Motta CCL, Crepaldi MA. O pai no parto e apoio emocional: a perspectiva da parturiente. Paidéia. 2005; 15(30):105-18.
17.García-Jordá D, Díaz-Bernal Z, Álamo MA. Legislación y atención medicalizada al nacimiento en el ejercicio de la maternidade y la paternidade em Cuba. Rev Cienc Salud. 2012; 10(2):207-21.
18.MacDorman MF, Mathews TJ, Declercq E. Home births in the United States, 1990–2009. NCHS Data Brief. 2012; 84:1-7.
19.Ministério da Saúde (Br). Departamento de Informática do SUS. [Internet]. Nascidos vivos. [cited on Jan 20, 2016]. Available from: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinasc/cnv/nvrn.def
20.Patah LEM, Malik AM. Modelos de assistência ao parto e taxa de cesárea em diferentes países. Rev Saúde Pública. 2011; 45(1):185-94.
21.Leister N, Riesgo MLG. Assistência ao parto: história oral de mulheres que deram à luz nas décadas de 1940 a 1980. Texto & contexto enferm. 2013; 22(1):166-74.
22.World Health Organization. Appropriate technology for birth. Lancet. 1985; 2(8452):436-7.
23.Kululanga LI, Malata A, Chirwa E, Sundby J. Malawian fathers' views and experiences of attending the birth of their children: a qualitative study. BMC Pregnancy and Childbirth. 2012; 12(141):1-10.
24.Caires TLG, Vargens OMC. A exclusão do pai da sala de parto: uma discussão de género e poder. Referência. 2012; 3(7):159-68.
25.Frank TC, Pelloso SM. A percepção dos profissionais sobre a assistência ao parto domiciliar planejado. Rev Gaúcha Enferm. 2013; 34(1):22-29.
26.Nascimento NM, Progianti JM, Novoa RI, Oliveira TR, Vargens OMC. Tecnologias não invasivas de cuidado no parto realizadas por enfermeiras: a percepção de mulheres. Esc Anna Nery (impr.) 2010; 14(3):456-61.
27.Gomes ML, Moura MAV. Modelo humanizado de atenção ao parto no Brasil: evidências na produção científica. Rev enferm UERJ. 2012; 20(2):248-53.