RESEARCH ARTICLES
Post-accident conducts by contact with biological material among workers in emergency medical service
Adriana Cristina OliveiraI; Maria Henriqueta Rocha Siqueira PaivaII
INurse. Post-Doctorate by the New York University, U.S.A. Associate Professor of the Nursing School of the Federal University of Minas Gerais. Researcher of the Conselho Nacional de Desenvolvimento Científico e Tecnológico. Leader of the Center for Studies and Research in Health Care Related to Infection. E-mail: adrianacoliveira@gmail.com
IINurse. Doctorate by the Post-Graduation Programo f the Nursing School of the Federal University of Minas Gerais. Nurse of the Emergency Mobile Care System of the Prefeitura Municipal of Belo Horizonte. Member of the Center for Studies and Research in Health Care related to Infection. E-mail: mariahenriquetarsp@yahoo.com.br
ABSTRACT: This research aimed at estimating the prevalence of accidents from exposure to biological material and post-accident conducts and serological follow-up for professionals from the Emergency Medical Services in Minas Gerais, Brazil. This cross-sectional study was undertaken from October, 2011 to July, 2012. Structured questionnaire, descriptive analysis, and analysis of prevalence were used. 487 professionals participated in the study; global prevalence of professionals injured was 17.0%, post-accident medical assessment occurred in 35.5% of cases, and mandatory accident report in only 29.7% of cases. The anti-HBV was undertaken in 13.2% of cases, anti-HCV in 9.1% and anti-HIV in 10.7%, both from the department and the professionals. Serologic follow-up for AIDS was conducted for 5.8% of cases, 4.9% for Hepatitis B, and 2.5% for Hepatitis C. These results are expected to stimulate discussion on the importance of reporting, evaluation, and monitoring of the professionals injured.
Keywords: Emergency medical services; accidents, occupational; prevention & control; occupational accidents registry.
INTRODUCTION
Health workers are exposed to biological agents, once routinely they are exposed to contact with blood and other organic fluids contaminated by a variety of potential pathogens related to occupational diseases. Usually such infectious diseases are associated with post-contact contamination with sharp objects containing blood or secretions and excretions spatter on mucous membranes and/or broken skin1.
Accidents with occupational exposure to biological material are frequent between workers of surgical and emergency area1,2-4. Among these professionals are those who carry out activities in pre-hospital care environments (PhE) by intense contact with bodily fluids related to the care of victims of trauma and clinical pictures up and by the complexity of activities aiming at stability and the maintenance of life5-9.
To prevent the transmission of occupational infections, the most effective way consists in adopting the standard precautions, engineering measures targeting the security of the devices used and analysis of occupational risks in the workplace10. Even like this, the possibility of exposure to biological material may be present and in these cases, the adoption of immediate pipelines, treatment and post-exposure follow-up can be decisive to minimize or avoid the acquisition of diseases to the detriment of the occupational accident3.
The occurrence of accidents by exposure to biological material among professionals of the PhE is not well known. In Brazil, besides the few studies that have examined the prevalence of these events5-9, not all assessed the immediate conduct and serological follow-up of injured professionals5,7,8, that constitutes an important knowledge gap.
In front of the above, it is proposed to estimate the prevalence of accidents by exposure to biological material, pipes and serological follow-up post-accidents of professionals in the pre-hospital care of the State of Minas Gerais.
LITERATURE REVIEW
Acquired Immunodeficiency Syndrome (AIDS) and hepatitis B and C are considered very important epidemiological diseases, mainly from the first proven case of seroconversion to the Human Immunodeficiency Virus (HIV) occurred after occupational exposure of a British nurse in 1984. The seroconversion of health workers accidentally post-contact with contaminated material by HIV/AIDS, hepatitis B virus (HBV) and C (HCV) has been recognized, proven and documented11-13.
In relation to the transmission of HIV it is estimated on average, that their risk is 0.3% in percutaneous accidents; 0.09% after exposures in mucous membranes; and involving not full skin are not enough data to quantify, but it is believed that the risk is lower than the exposure on mucous membranes. Since the beginning of the AIDS epidemic in 1981 until 2002, 106 cases were proven and 238 probable cases of HIV infected health professionals by accidents at work were published around the world. Most cases of HIV seroconversion, involved large amount of biological material inoculated with caliber needles, causing deep lesions and spontaneous bleeding in the injured professional3,11-13.
As for the hepatitis B virus, it is estimated that it is responsible for a million deaths/year and that currently there are 350 million chronic carriers in the world. The stability of the virus, the different forms of transmission and the existence of chronic carriers allow the survival and persistence of HBV in the population2,14.
The hepatitis C virus was identified in 1989 and serological tests for the detection of this virus became available from 1992. It presents important variability in its genome, due to frequent mutations during the viral replication process. Both the chronic infections as the acute are usually asymptomatic, which slows down considerably the diagnosis of the disease. The period of evolution of hepatitis C is long and can reach 30 years, with possibility of developing liver cirrhosis and hepatocellular carcinoma. It is estimated that there are 170 million people infected around the world14.
METHODOLOGY
This is a descriptive study of transverse design conducted with public service professional of the Urgency Mobile Service of nine municipalities in the State of Minas Gerais in the Southeast region, where this mode of healthcare is deployed for over a year and covers a population of more than 100,000 inhabitants. The criteria for selection of the municipalities is supported on the principles recommended by Ordinance No. 2,048/2002 of the Ministry of Health for the operation of the services of PhE15.
The eligible subjects for this study were physicians, nurses, technicians and nursing assistants and drivers operating in mobile units and were direct service to the user of this service for over a year.
We used a structured questionnaire that contemplated demographic and professional issues (professional category, sex, age, time of performance in institution, stocking unit, number of bonds and weekly work days), the occurrence of the accident, ducts, serological monitoring professional post-accident behavior and the accident ranked mucous, percutaneous and not full skin according to the Manual of recommendations for care and monitoring of occupational exposure to biological material from the Ministry of Health (MH)4.
The analysis of post-accident behavior and serological follow-up of the injured professional were conducted in two distinct forms:
For the invitation to the services, the consent of the local coordination of each municipality was asked and after the acceptance, the direct contact with each professional for presentation of the objectives of the study, stressing the importance of the results for the deepening and the knowledge of this topic and the possible repercussions for the health of the worker. That same opportunity, after research participate in acquiescence, the Informed Consent (TFCC) was presented and signed by the participants.
The data collection was conducted between December 2011 and July 2012 and referred to occupational exposures occurred in the 12 months preceding data collection. The data collected were entered into Excel spreadsheet and its analysis was performed on Statistical Package for Social Science(SPSS) version 18.0.
The characterization of the population, the specification of the immediate post-accident behavior and serological monitoring of professional accident were checked by calculating absolute frequencies and percentages. After the analysis of the distribution of quantitative variables, they were dichotomized using as point cutting the value of its medians.
The research project was based on resolution No. 196/96 of the National Health Council, submitted to the Research Ethics Committee of the Federal University of Minas Gerais and approved by Opinion No. 503/ETIC 2011.
RESULTS AND DISCUSSION
The population of this study was composed of 487 respondents included doctors (25.5%), nurses (12.3%), nursing technicians (35.5%) and drivers (26.7%). The global prevalence of injured professionals with exposure to biological material (BM) was 17.0% (83/487), and 47.9% percutaneous contact involved; 39.7% for mucous membranes and 12.4% not full skin. Among the injured workers, 67.5% (56/83) reported a single exposure to biological material; for 19.3% (16/83), two; and three to 13.2% (11/83), totaling 121 occupational accidents in the period analyzed.
The global prevalence of accidents at work involving BM in this study, was lower than the observed in studies conducted with professionals of the PhE of two other cities in the State of Minas Gerais where 19.8 to 20.6%6,9; among paramedics in the United States, 21.6%16 and among professionals of the Fire Brigade of a municipality in Central Goiás State, Brazil, 40%17.
Generally speaking in this study, workers reported that the post-accident medical evaluation was carried out in 35.5% (43/121) of exposures by an enabled professional; and to 29.7% (36/121) of all cases the notice of accident at work was issued (NAW).
In relation to medical consultation specialized and consequent issue of post-accident work accident release, surveys conducted with professionals of the PhE of other cities of the States of Minas Gerais and Goiás strengthened the results obtained by this study registering an average of 22.7% (None – 36.7% of cases) for medical evaluation and an average of 9.0% (None -18.4% of cases) for the issue of NAW considered mandatory character6,9,17.
The post-accident medical evaluation is essential to analyze the severity of exposure, serologic tests request for hepatitis B, C and HIV, prescription and chemoprophylaxis indication4. The nonfulfillment of the NAW detracts possibility of associating exposure to the likelihood of the development of occupational disease, as well as underestimate the real statistic of occupational exposures to BM between health workers.
Although considerable progress has been noted in relation to the understanding on the occupational risk and the possibility on developing some diseases spread by bodily fluids after accidental contact, health workers still are resistant against post-accident assessment and notification of accidents at work and consequently underestimate the risk of infecting18.
The occupational accident should be reported immediately after its occurrence, through the issuance of (NAW)19 which despite being legally binding, in practice the underreporting of occupational accidents is observed6,9,17.
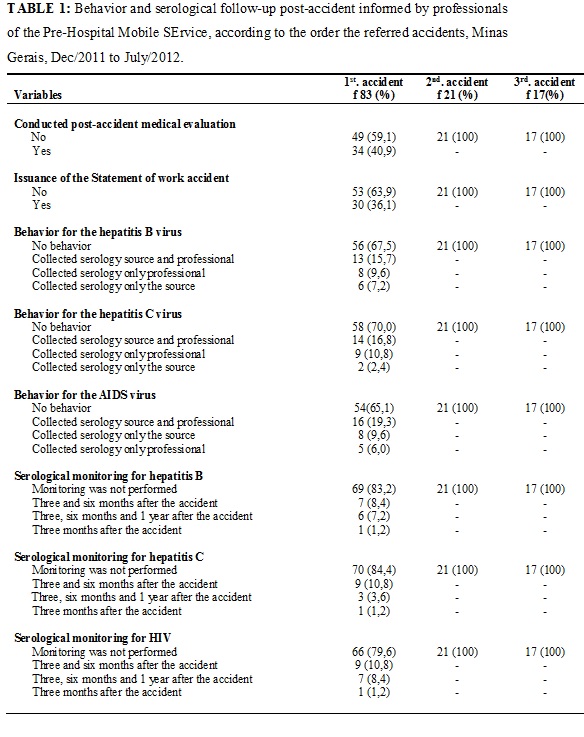
In this study, at the time of the accident, in relation to the recommendation to perform serology for hepatitis B, C and HIV, both as professional source, it was found that for 10.7% (13/121) of the cases the anti-HBV has been performed. To 9.1% (11/121) of cases, the participants also reported making the anti-HCV and 13.2% (16/121) to HbsAg. For hepatitis B, it was found that 4.9% (6/121) of professional accidents were accompanied by one year after the occurrence of exposure to biological material; 2.5% (121/03) for hepatitis C; and 5.8% (07/121) for HIV.
The results recorded in relation to behavior and serological monitoring for the possibility of occupational transmission of hepatitis B, C and HIV in PhE professionals, according to the order of these accidents are shown in table 1.
Finally, we evaluated the behavior and serological monitoring in post-accident care workers of the Pre-Mobile Hospital Care Service in the State of Minas Gerais, according to the type of accident. The results are in Table 2.
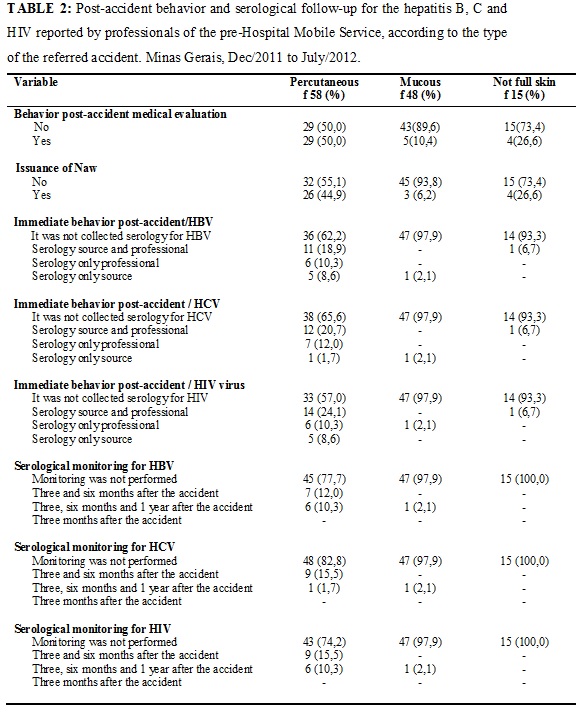
The professionals who have had contact with percutaneous biological material were those who reported the highest rates of post-accident behavior and serological follow-up when compared to other types of exposure, according to the table 2.
In addition to the underreporting of accidents with biological material exposure, in this study we also observed that almost all the workers was not evaluated in a second and third contact with BM. In relation to the type of accident, it was found that the assessment and issuing of the NAW were higher when the accident occurred percutaneous or full skin, to the detriment of the guidance of the Ministry of health, where contacts of BM with mucous membranes are recognized as more serious when compared to the contact with full skin3.
It seems to exist between health professionals a belief that the occupational accident with biological material exposure is a phenomenon inherent to the profession, it is a risk that will always be present regardless of the measures applied to minimize it. Also in practice routine is to note that many workers only use personal protective equipment (PPE) when they know that the patient is a carrier of a communicable disease, underestimating this possibility when there is this information.
Work accidents involving blood and other potentially contaminated fluids should be treated as an emergency measure, since the interventions for prophylaxis of HIV infection and hepatitis need to be initiated shortly after the occurrence of the accident, preferably two hours post-exposure only and should not exceed the maximum period of 72 hours. This behavior enhances the effectiveness of treatment and may inhibit viral replication and therefore, reduce the amount of circulating virus3.
After an occupational exposure to biological material it is recommended to wash with soap and water, and if the mucosa is the exposed area, the washing should be exhaustive with water or saline solution6. Despite this guidance, such behavior is not always performed by professionals, casualties unknown low credibility, infrastructure or neglect. Thus, a variety of behavior has been logged20-22 and in some situations, as in the pre-hospital care, not always the professional offers suitable location, with sink and water for this activity, at the time of the accident.
Some studies have proposed to establish correlation between occupational accident and seroconversion to hepatitis B and C. However, this objective has not been achieved owing to the ignorance, in most cases, the situation previous serological of professionals and of possible risk conduct adopted as unprotected sex, heterosexual with multiple partners and sex with sex workers without protection, registration of blood transfusions, intravenous drug use or hemodialysis, among other22.23.
In this sense, the difficulty in establishing an association between occupational exposure and seroconversion to these diseases may be added to the neglect of the worker and the institution evidenced by lack of incentive policies to vaccination, follow-up to the serological status of the professional, the notification of the accident and its follow-up for the period recommended by the Ministry of Health in the guide Recommendations for care and monitoring of occupational exposure to biological material: HIV and hepatitis B and C4.
In relation to the behavior post-accident, a given concern has been observed in studies with health professionals who carry out assistance in emergency conditions which notification of accidents at work is not always carried out, resulting in ignorance of the real magnitude of accidents. In this way, potential damage to the health of the worker may be caused in the long term, making it impossible for the establishment between the causal agent and the development of diseases, as well as the legal protection in relation to the industrial accident, 6,7,9.
On the other hand, it calls attention to the lack of incentive policies to the notification of the accident. Accident communication stems from a spontaneous attitude of the worker to reflect about their own safety. Between emergency services professionals, it is possible to check often a misguided practice, in which the worker associates the occurrence of the accident to an event expected by the performance of the professional activity, belittling their risk of acquisition of potential diseases and especially its legal protection in case of seroconversion.
CONCLUSION
The global incidence of accidents at work involving biological material in the year 2010 was 26.1%, highlighting their occurrence among the nursing technicians and doctors.
Globally, it was found that a small portion of injured workers conducted post-accident medical assessment and subsequent issuance of NAW, quick test for HIV and for hepatitis B and C. As for the serologies regarding follow-up serologic, due to the possibility of transmission of hepatitis B, C and HIV for a year, found herself an even smaller membership.
The analysis of behavior and serological follow-up after each occupational accident by exposure to biological material that revealed a low ratio for a first accident, however for a second or third these were insignificant.
Regarding the analysis of the types of occupational accidents involving contact with biological material, it was observed that most professionals said having immediate behavior and accomplished serological follow-up indicated when the exhibition was at the expense of percutaneous other types.
Taking into consideration that the occupational accident cannot always be avoided and that the trader can ignore the guidelines recommended by the Ministry of Health for this type of event, it becomes vital that this information is disseminated in scientific meetings, lectures, discussions and clinics posted in areas of movement for workers. Must still be passed on in professional education programs, the dissemination of information and flowcharts about the professional forwarding exposed to biological material, an indication of the need of serologic testing for HIV, HBV and HCV, the identification of basic health units and ER units that perform this staff.
REFERENCES
1. Gerberding JL. Occupational exposure to HIV in health care settings. N Engl J Med. 2003; 348: 826-33.
2. Siegel JD, Rhinehart E, Jackson M, Chiarello L. The Healthcare Infection Control Practices Advisory Committee, 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, June 2007. [Citado em 10 dez 2013] Available at: http://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf
3. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Exposição a materiais biológicos. Brasília (DF): Editora MS; 2006.
4. Ministério da Saúde (Br). Programa Nacional DST/AIDS. Secretaria de Vigilância em Saúde. Programa Nacional para a Prevenção e o Controle das Hepatites Virais. Departamento de Vigilância Epidemiológica Secretaria de Vigilância em Saúde. Recomendações para atendimento e acompanhamento de exposição ocupacional a material biológico: HIV e Hepatite B e C. Brasília (DF): Editora MS; 2004.
5. Zapparoli AS, Marziale MHP. Risco ocupacional em unidades de suporte básico e avançado de vida em emergências. Rev Bras Enferm. 2006; 59: 41-6.
6. Oliveira AC, Lopes ACS, Paiva MHRS. Acidentes ocupacionais por exposição a material biológico entre a equipe multiprofissional do atendimento pré-hospitalar. Rev esc enfer USP. 2009; 43: 677-83.
7. Soerensen AA, Moriya TM, Hayashida M, Robazzi MLCC. Acidentes com material biológico em profissionais do Atendimento Pré-hospitalar Móvel. R enferm UERJ. 2009; 17: 234-9.
8. Vegian CFL, Monteiro MI. Living and working conditions of the professionals of the a mobile emergency service. Rev Latino-Am Enfermagem. 2011; 19: 1018-24.
9. Paiva MHRS, Oliveira AC. Fatores determinantes e condutas pós-acidente com material biológico entre profissionais do atendimento pré-hospitalar. Rev Bras Enferm. 2011; 64: 268-73.
10. U.S. Public Health Service. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. MMWR Recomm Rep.2001; 50(RR-11):1-52.
11. Cardo DM, Culver DH, Ciesielski CA, Srivastava PU, Marcus R, Abiteboul D, et al. Case-control study of HIV seroconversion in health care workers after percutaneous exposure. N Engl J Med. 1997; 337: 1485-90.
12. Centers for Disease Control. CDC. Case control study of HIV serocon-version in health-care workers after percutaneous exposure to HIV-infected blood. MMWRRecomm Rep. 1995; 44: 929-33.
13. Corey KE, Servoss JC, Casson DR, Kim AY, Robbins GK, Franzini J, et al. Pilot study of postexposure prophylaxis for hepatitis C virus in healthcare workers. Infect Control Hosp Epidemiol. 2009; 30: 1000-5.
14. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias. 3ª Ed. Guia de Bolso. Brasília (DF): 2010.
15. Ministério da Saúde (Br). Regulamento técnico dos Sistemas Estaduais de urgência e emergência. Portaria GM/MS 2.048, de 5 de set. 2002. Brasília (DF): Gabinete Ministerial; 2002.
16. Leiss JK, Ratcliffe JM, Lyden JT, Sousa S, Orelien JG, Boal WL, et al. Blood Exposure among paramedics: incidence rates from the National Study to Prevent Blood Exposure in Paramedics. Annals of Epidemiology. 2006; 16(9): 720-5.
17. Florêncio VB, Rodrigues CA, Pereira MS, Souza ACS. Adesão às precauções padrão entre os profissionais da equipe de resgate pré-hospitalar do Corpo de Bombeiros de Goiás. Rev Eletrônica Enferm. 2003; 5(1). [citado em 10 dez 2013] Available at: http://www.fen.ufg.br/revista/re vista5_1/adesao.html
18. Damasceno AP, Pereira MS, Souza ACS, Tipple AFV, Prado MA. Acidentes ocupacionais com material biológico: a percepção do profissional acidentado. Rev Bras Enferm. 2006; 59: 72-7.
19. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Notificações de Acidentes do Trabalho Fatais, Graves e com Crianças e Adolescentes. Brasília (DF); Editora MS; 2006.
20. Garcia LP, Blank VLG. Condutas pós-exposição ocupacional a material biológico na odontologia. Rev Saude Publica. 2008; 42: 279-86.
21. Teixeira CS, Pasternak-Júnior B, Silva-Sousa YTC, Correa-Silva SR. Medidas de prevenção pré e pós-exposição a acidentes perfurocortantes na prática odontológica. Rev odonto cienc. 2008; 23(1): 10-4.
22. Fligner DJ, Wigder HN, Harter PM, Fliegelman RM, Jewell M, Perlman P. The prevalence of hepatitis b serologic markers in Suburban paramedics. J Emerg Med. 1989; 7(1): 41-5.
23. Wergman HA, Gwinn R. Seroprevalence of Hepatitis B and Hepatitis C among rural emergency medical care personnel. Am J Emerg Med. 1997; 15: 248-51.