RESEARCH ARTICLES
Directly observed treatment of tuberculosis: learning process in a higher education institution
Rafaella GreccoI; Cassiara Boeno Borges de OliveiraII; Laís Mara Caetano da SilvaIII; Káren Mendes Jorge de SouzaIV; Glauber Palha dos SantosV; Pedro Fredemir PalhaVI
IUndergraduate, Bachelor of Nursing, Nursing School of Ribeirao Preto, University of Sao Paulo. Ribeirao Preto, Sao Paulo, Brazil. Email: rafaella.grecco@usp.br.
IIDoctoral Student of the Graduate Nursing Public Health Nursing, School of Nursing of Ribeirao Preto, University of Sao Paulo, Ribeirao Preto, Sao Paulo, Brazil. Email: cassiara.boeno@gmail.com.
IIDoctoral Student Graduate in Public Health Nursing, School of Nursing of Ribeirao Preto, University of Sao Paulo. Ribeirao Preto, Sao Paulo, Brazil. Email: laismara@eerp.usp.br.
IVPhD in Science. Student at the School of Nursing at the State University of Rio de Janeiro, Brazil, Email: karenmjs@hotmail.com.
VMaster's Student Graduate in Public Health Nursing, School of Nursing of Ribeirao Preto, University of Sao Paulo. Ribeirao Preto, Sao Paulo, Brazil. Email: glauber.palha@gmail.com.
VIPhD. in Nursing, Associate Professor, Department of Maternal-Child Nursing and Public Health Nursing School of Ribeirao Preto, University of Sao Paulo. Ribeirao Preto, Sao Paulo, Brazil. Email: palha@eerp.usp.br.
VIIArticle extracted from scientific research project linked to the Exchange Teaching with Research, produced from the multicentric project DOTS Strategy in the treatment of tuberculosis: performance of Primary Care in municipalities of South, Southeast and Northeast of Brazil, Universal Notice nº 14/2010 of the National Council for Scientific and Technological Development.
ABSTRACT: This quanti-qualitative study examined theoretical and practical learning processes among undergraduate nursing students at a public institution in Ribeirao Preto, Sao Paulo, as regards the Directly Observed Treatment of tuberculosis. Data were collected in 2011 using a self-administered questionnaire of five questions and were analyzed, respectively, using descriptive statistics and the analytical theory of Collective Subject Discourse. It was observed that most of the 72 respondents had no contact with DOTS during the course and that the limited knowledge displayed was shaped by the hegemonic model of health care. It was concluded that better coordination between education activities relating to tuberculosis and to directly-observed treatmentis needed in the training process for generalist nurses, given that they have specific attributes in care management and care for tuberculosis patients, relatives and other contacts.
Keywords: Nursing education; human resources; directly observed therapy; tuberculosis.
INTRODUCTION
Tuberculosis (TB) is a disease with a significant magnitudeVII, historically overlooked in the public policy agenda, in part, by the illusion that this health problem, configured as a misunderstanding, would be controlled or even solved1. Some of the data corroborated this statement, such as the occurrence of 9.3 million new cases of the disease in the world2, as well as the 19th position occupied by Brazil among the 22 countries responsible for 80% of the global burden of the disease3.
In order to reverse this situation, in 1993, TB was declared as world emergency recommending the strategy Directly Observed Treatment Short-Course (DOTS) as a response to its control2. Among these, the directly observed treatment (DOT) is characterized as a key element, with a view to strengthening adherence to treatment and the prevention of the emergence of strains resistant to medicines3.
perationally, it consists in ensuring the regular chemotherapy and correct requiring, for both, supervision of daily ingestion of medicines4.
One must consider the following treatment modalities: home (supervised of patient residence or place indicated by him); health unit (basic health units (BHU), family basic health units (FBHU), answering services people living with human immunodeficiency virus and acquired immunodeficiency syndrome (HIV/AIDS) (specialized clinics or hospitals); prison (prison system) or shared (conducted in two health units, and in one it gives medical consultation and another closer to the patient's residence, or DOT)5.
The therapeutic modality choice is very important and should be guided in a joint fashion, between the healthcare team and the patient. However, the logic of organization in several departments of attention to TB follows strict rules6, which are established by international epidemiological methods, establishing disease control and especially the patient not considering the autonomy of this subject in the care process of the therapy. It is understood that, for which there is no autonomy of the patient in relation to its treatment, it is necessary to build a bond between the TB patients and healthcare services5.
Regarding this important element of TB control - DOT - stands out its space in the teaching learning process in Higher Education Institutions (HEIs) to be committed to the training of qualified human resources to respond to the demands of the system Unified Health System (UHS) and also to its principles, such as equity, universality and comprehensiveness.
Thus, this research is justified in view of the relevance of the issue facing the nursing education - especially at the higher level of education - with a view to strengthening the practices of health promotion and disease prevention, in particular for TB. Therefore, we aimed to analyze the theoretical and practical learning processes related to DOT for TB, experienced among nursing undergraduates of a public higher education institution in Ribeirao Preto, Sao Paulo, Brazil.
LITERATURE REVIEW
We performed a review of the literature between the months of April and May 2012, in the following databases, Latin American and Caribbean Literature in Health Sciences (LILACS) and Medical Literature Analyzes and Retrieval System (MEDLINE) via Pubmed. The following controlled descriptors were used: tuberculosis, directly observed treatment, human resources and nursing education. As inclusion criteria, it was considered whether the use of original articles published in the last five years that sensitively addressed the central theme of the study.
From this, 16 articles were selected, and only one spoke specifically about the issue of the teaching of TB in the undergraduate training process. This, in turn, showed that the transmission of knowledge in relation to the disease and DOT occurred so verticalized, reality that was stagnant learning, a time that were not given an opportunity in discussions and formulations of critical opinions about the theme7.
Because of the limited literature and the relevance of this theme, especially in what concerns the educational policies related to TB and the DOT, this research it configures itself as of paramount importance to the dissemination of this knowledge, as well as for incitement for new discussions of the IES Brazilian political-pedagogical projects.
METHODOLOGY
This is a descriptive study with a qualitative approach. The study population consisted of undergraduate nursing students from a public IES the city of Ribeirao Preto, which were in the last period of the course and supervised practice, total - according to data from that institution - 118 students. Participants were automatically excluded, who did not confirm acceptance after three attempts to contact via email or phone as well as those who agreed to participate, but not correctly filled out the Statement of Informed Consent Form (SICF), or did not return the data collection instrument. Following these criteria, this study comprised 72 subjects.
Data collection occurred between the months of August and September of 2011, by means of a self-applied instrument containing five questions, being three closed and two open. The closed questions addressed the personal characteristics of students (gender, age, modality - Bachelor's Degree or a Bachelor's and Master's Degree - and period of course), and the existence or not of contact with the DOT during their graduation. The open questions, in turn, were related to the guidelines provided by undergraduates to TB patients in relation to DOT and the perceptions of students about this therapeutic strategy.
For the analysis of quantitative data, statistical techniques used were descriptive (analysis of simple frequency and construction of tables), by means of thesoftware Statistic 9.0, the Statsoft. Inc. The qualitative analysis made use of the methodological strategy and analytical of collective subject discourse (CSD), which aims to extract from each testimonial central ideas (CI) with their respective key-expressions (KE) similar, making possible the composition of one or more speeches-summaries in the first person singular. This analytical method allows to produce collective opinions drawing on individual opinions, still observing the frequency with which they appear8.
In this respect it should be noted that, of the 72 respondents, 39 answered the open questions of the instrument, which enabled the elaboration of two IC, the first being A DOT is a systematic treatment, in which are prioritized guidelines on pharmacological therapy, follow-up of treatment and signs and symptoms of TB, related to the first open question of instrument - That guidelines were given to patients during the administration of the DOT? The second IC formulated was The DOT is characterized as being a fundamental strategy for the realization of the cure of TB, referring to the second open question of instrument - what do you think about the DOT?. With the aim of guaranteeing the anonymity of the interviewees, the participants of this study were represented by five CSD, which are, CSD1, CSD2, CSD3, CSD4 and CSD5.
It is worth noting that this study was submitted to and approved by the ethics in Research Committee of the School of Nursing of Ribeirao Preto, University of Sao Paulo (RC/SNRP/USP), according to the protocol no. 1264/2011, in order to meet the Resolution no. 196/969 of the National Health Council (NHC).
RESULTS AND DISCUSSION
This research counted with the participation of 72 nursing graduates, and of these 71 were female and one male. The age ranged between 20 and 32 years, with a mean age of 23.3 years. As for the undergraduate course, 53 subjects belonged to a Bachelor's Degree - with duration of 4 years - and 19 were enrolled in the Undergraduate and Graduate, with duration of 5 years.
It is worth pointing out that the whole person, by right guaranteed, you can enjoy the highest level of physical and mental health, clearly highlighted in the Code of ethics of the International Council of nurses10, which governs the nursing profession in the world. However, for this legitimate power is in fact fulfilled, you must assume it as social commitment since the beginning of the professional training of nurses11.
In fact, TB control, sustained under three main focuses - detection of new cases, early diagnosis and appropriate treatment - also is characterized as a right to healthcare, especially in relation to the DOT. This aims at strengthening the accession of ill treatment and the prevention of the emergence of resistant strains to medicines, thus reducing the cases of abandonment and increasing the likelihood of cure5.
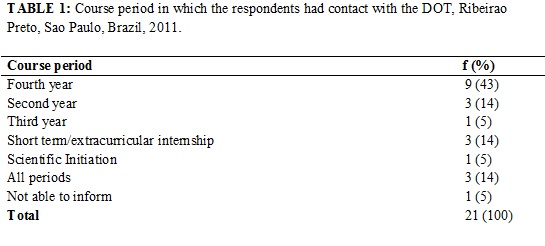
About this, it was possible to identify in this study that the majority of participants, 51 (70.84%), had no contact with the theme of DOT during the undergraduate course. Consequently, many did not know about the use of this strategy for the control of TB and, among the 21 (which represented 29.16%) who reported having been contact, it is identified predominance - 9 (43%) - the answer in the last year of academic training, as shown in Table 1.
This fact is considered worrying, especially because of the professional nurse - especially those who work in primary health care (PHC) - hopes to assumption of responsibilities along the actions of prevention and control of the disease, which must be guided by means of appropriate planning of interventions integrals (political, economic and health), assuming primarily from the local context11. In addition, a study revealed that nursing students over the course of graduate studies if they expose greatly to the risk of contagion infectious diseases, among these are TB. This exposure occurs mainly by students of misinformation regarding the biosafety norms and the ignorance of basic concepts about the disease and its forms of contagion12.
The encounter of these data, it was possible to observe even the CSD constructed from the reports of 21 undergraduates to issue guidelines, which were given to the patients during the administration of the DOT? Where two categories (A and B) can distinguished, respectively named: Guidelines on medication, side effects, importance and continuity of treatment; and guidelines about signs and symptoms of the disease and on the forthcoming medical consultations. In these, it was possible to observe aspects related to hegemonic model of healthcare, disarticulated, therefore, the practice of health promotion and disease prevention, which express the pillars of PHC. In This way, the following are the categories and their respective CSD.
Category A: guidance on medication, side effects, importance and continuity of treatment
I Advised about the medication, when and how to administer, if taken properly, preferably in fasting. I said that it is important to continue treatment and that he should take the medication regularly, because the treatment should not be interrupted. I mentioned that he should continue the treatment even in the absence of signs and symptoms, informed about the adverse reactions and about the possible side effects of medicines. (CSD1, constructed from the responses of 6 subjects).
Category B: Guidelines about signs and symptoms of the disease and on the forthcoming medical consultations
I gave information regarding signs and symptoms of the disease, examination, medical consultation, procedures for sputum smear microscopy of control (collection of samples). I instructed the benefits that patients have the right (basic food basket) and about upcoming medical appointments. (CSD2, constructed from the answers of 4 subjects).
These aspects may be reflections of a nursing education that calls other discussions in academia, including the experience of extended concepts and the development of comprehensive care as one of the guiding principles in health practices, providing the user/patient an effective participation in their treatment plan13. To encounter this affirmative, study14 showed distancing between the education offered by universities and the real health needs of the population, a fact that can still be modified if, however, the content-paradigms still prevalent in educational institutions.
Given that, the area of nursing back its activities mainly to the care of people, the process for these professionals is grounded in human contact and the relationship between them. Thus, this ratifies the idea, the university evocation a fundamental role in the training of professionals imbued with scientific and technical knowledge, but above all, humanitarian with a view to improving the quality of life and health of the population15.
With the advent of the Brazilian Sanitary Reform and the formulation of UHS in the Constitution of 198816, the health professionals and the population began to be seen as active subjects of the health-disease process. Disease, from this moment, becomes not be more the single focus of observation, but the understanding of the way of life, as well as the working conditions of these individuals/social groups, and consequently as this whole process resonates in their health14.
It is expected, therefore, that the nurse proves sympathetic to the problems reported by patients of TB in DOT, creating a relationship such that it is able to facilitate the sharing of responsibilities with the operationalization of therapy, not only informative, with remnants the authoritarian character of the hegemonic guided care model. These aspects, which were observed in CSD constructed from the reports of 39 students to question what do you think about the DOT?, which originated, by its turn, three categories (C, D and E) respectively denominated: important strategy for TB control; enables evaluation of treatment; and accession and abandonment to the treatment. Here are the categories and their respective CSD.
Category C: Important strategy for tuberculosis control
I think it is very important for the reduction of rates of tuberculosis; already that supervision is very important for the success of the treatment. Furthermore, it is a way to monitor closely the development of the patient, characterizing it as an effective strategy for a better control of diseases with major repercussions as the TB. Therefore, I think it is essential as a means of effective control. (CSD3, constructed from the discourse of 5 subjects).
Category D: Enables evaluation of treatment
It is important to assess whether the patient is actually performing the appropriate treatment for the disease. The supervision is very important, because some patients can't keep pace with the treatment correctly, being important for both prevention as for the recovery of the patient. (CSD4, constructed from the answers of 4 subjects).
Category E: adherence and abandonment of treatment
I think it is important to allow adherence and efficacy of tuberculosis treatment. It seems to be interesting to ensure the correct treatment, since the patient's follow-up to treatment in an appropriate manner. These factors decrease the chances of the patient leaving the treatment, once the treatment is too long and often leads to withdrawal on the part of the patient, because when you begin to feel better he has a tendency to abandon treatment. (CSD5, constructed from the responses of 7 subjects).
It is necessary to rethink the educational practices more broadly related to TB and DOT within curriculum, especially taking into account that the context in which is located the EIS - scenario of this research - is taken as priority for control of the disease, there is no view of the high number of cases (196 cases/year), with incidence rate of 35 cases/100,000 inhabitants in the past 9 years17. This, therefore, corroborates the National Curricular Guidelines (NCG) of nursing courses, which guide that the formation of this professional should contemplate the acquisition of competences and skills, whereas the epidemiological picture of the country/region and the real needs of the community18.
Another important fact was related to professionals who have provided guidance to TB patients at the time of completion of the DOT, who in their majority were performed by professionals from the middle, as demonstration of Table 2.
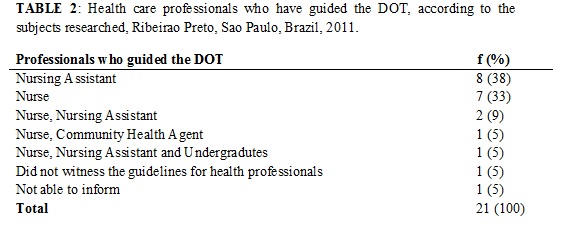
In accordance with the expected competencies of nurses in relation to the shares of supervision, coordination and permanent educational activities19, it is understood that this therapeutic modality, preferably, should be performed under the supervision of this professional. However, compared to the current context of health practices in the PHC, it is understood that it is necessary to rethink the shared management with a view for conducting supervised therapy by other professional health team or family members properly trained for this task.
It should also be highlighted that the permanent education plays its role only when involved in a transformative praxis, which translates to a dialectical theory of knowledge as a process of creation and recreation, developing critical reflection about their work20. This is reflected in greater humanization in the care, improving the quality of the attention paid by UHS, both in technical content as the contact of the professionals with the population that uses these services.
Based on these, it is inferred that the integration of theory and practice in health will be satisfactory fact that the various subjects involved in training (teachers, students and working professionals in health services) are receptive to the understanding and experiencing and promoting horizontalization of knowledge. For this purpose, it is necessary to aim at the training of professionals not only technical, but also able to perform activities previously not required, as the action with the population, and institutional organs of public administration groups. Therefore, it is expected that these actors can develop their work articulating complementary knowledge, to meet the needs of the population, to reflect their on practices and evaluate the entire healthcare process14,21.
CONCLUSION
Greater articulation of educational practices related to TB and DOT in the training process of the generalist nurse, considering that this professional has specific attributes in managed care and assistance to TB patients, their families and other communicators is required. Thus, it becomes necessary educational practice guided by the incorporation of innovative learning processes and problem solving, with the aim of offering subsidies needed to improve the qualification of health professionals at tertiary level, aimed at strengthening the practices of disease prevention and promote the health of the entire population.
The limitations of this study, there is the possibility of information bias, given that self-administered questionnaires were given to the study subjects, during meetings of intern groups in the presence of the responsible teachers. In addition, it is acknowledged that the limited sample and single scenario can prevent the generalization of the findings.
Still, it is worth pointing out that although efforts in order to ensure the participation of all students in this study, there was a loss in the number of subjects, a fact that may be related to the gaps in the learning process of the sample, especially in what concerns the issue of TB.
REFERENCES
1. Hino P, Cunha TN, Villa TCS, Santos CB. Profile of new cases of tuberculosis in Ribeirao Preto, São Paulo State, in the period of 2000 to 2006. Ciênc saúde coletiva. 2011; 16: 1295-301.
2. World Health Organization. Global tuberculosis control 2004: epidemiology, strategy, financing. Geneva (Swi): WHO; 2009.
3. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Programa Nacional de Controle da Tuberculose. Manual de recomendações para o controle da tuberculose no Brasil. Brasília (DF): Ministério da Saúde; 2010.
4. Santos TMMG, Nogueira LT, Santos LNM, Costa CM. O acesso ao diagnóstico e ao tratamento de tuberculose em uma capital no interior brasileiro. Rev enferm UERJ. 2012; 20: 300-5.
5. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Programa Nacional de Controle da Tuberculose. Manual de recomendações para o controle da tuberculose no Brasil. Brasília (DF): Ministério da Saúde; 2011.
6. Brunello MEF, Cerqueira DF, Pinto IC, Arcênio RA, Gonzales RIC, Villa TCS, Scatena LM. Interaction between patient and health care professionals in the management of tuberculosis. Acta Paul Enferm. 2009; 22: 176-82.
7. Villa TCS, Ruffino-Netto A, Andrade RLP, Alarcón EA, Montero CV, Firmino DR. Survey on tuberculosis teaching in brazilian nursing schools, 2004. Int J Tuberc Lung Dis. 2006; 10: 323-7.
8. Lefèvre F, Lefèvre AMC. O discurso do sujeito coletivo: um novo enfoque em pesquisa qualitativa. Caxias do Sul (RS): Educs; 2003.
9. Ministério da Saúde (Br). Conselho Nacional de Saúde. Comissão Nacional de Ética em Pesquisa. Resolução nº 196 de 10 de outubro de 1996: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF): CNS; 1996.
10. Consejo Internacional de Enfermeras, editors. Código Deontológico del CIE para la profesión de Enfermería. Ginebra: Fornara; 2006 [citado em 19 jan 2014].
Available at: http://www.icn.ch/es/about-icn/code-of-ethics-for-nurses/#search=%22%22codigo%20del%20cie%22%2
11. Musayón Y, Loncharich N, Salazar ME, David HML, Silva I, Velásquez D. Nursing s role in tuberculosis control: a discussion from the perpective of equity. Rev Latino-Am Enfermagem. 2010; 18: 130-8.
12. Moreira MAC, Nápole RG, Silva VN. Perfil da resposta à prova tuberculínica em estudantes de enfermagem. Rev enferm UERJ. 2007; 15: 387-92.
13. Corbellini VL, Medeiros MF. Fragments of history: the nurse becoming a subject of herself. Rev Bras Enferm. 2006; 59: 397-402.
14. Chiesa AM, Nascimento DDG, Braccialli LAD, Oliveira MAC, Ciampone, MHT. A formação de profissionais de saúde: aprendizagem significativa à luz da promoção da saúde. Cogitare Enferm. 2007; 12: 236-40.
15. Borges AG, Vannuchi MTO, Durán González A, Vannuchi RO. Caracterização e expectativas de estudantes ingressantes de um curso de graduação em enfermagem. Espaço Saúde. 2010; 12:1-6.
16. Constituição 1988 (Br). Constituição da Republica Federativa do Brasil. Brasília (DF): Senado; 1988. [citado em 19 jan 2014]. Available at: http://www.planalto.gov.br/ccivil_03/constituicao/constituicao.htm
17. Secretaria Municipal de Saúde (RP). Assistência ao paciente com tuberculose em Ribeirão Preto. Ribeirão Preto (SP): Secretaria de Saúde; 2012. [citado em 12 jan 2013]. Available at: http://www.ribeiraopreto.sp.gov.br/ssaude/programas/tuberculose/i16assistencia.php
18. Conselho Nacional de Educação (Br). Câmara de Educação Superior. Resolução CNE/CES nº 3, de 7 de novembro de 2001. Institui Diretrizes Curriculares Nacionais do Curso de Graduação em Enfermagem. Diário Oficial da República Federativa do Brasil, Brasília (DF); 2001 nov 9; Seção 1: 37.
19. Ministério da Saúde (Br). Portaria nº 648, de 28 de março de 2006. Política Nacional de Atenção Básica: estabelecendo a revisão de diretrizes e normas para a organização da Atenção Básica para o Programa Saúde da Família (PSF) e o Programa de Agentes Comunitários de Saúde (PACS). Brasília (DF): Editora MS; 2006.
20. Ministério da Saúde (Br). Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Educação Permanente. Brasília (DF): Ministério da Saúde; 2000.
21. Santos JLF, Westphal MF. Práticas emergentes de um novo paradigma de saúde: o papel da universidade. Estudos Avançados. 1999; 13: 71-88.