RESEARCH ARTICLES
Comparison of quality of life domains in patients with venous ulcer
Gilson de Vasconcelos TorresI; Lívia Sêmele Câmara BalduinoII; Isabelle Katherinne Fernandes CostaIII; Felismina Rosa Parreira MendesIV; Quinídia Lúcia Duarte de Almeida Quithé de VasconcelosV
I
Nurse. Doctor in Nursing. Titular Professor of the Nursing Department of the Federal University of Rio Grande do Norte. Coordinator of the Research Group
Incubator of Nursing Procedures. Scholarship of the do Conselho Nacional de Desenvolvimento Científico e Tecnológico. Natal, Rio Grande do Norte, Brazil.
E-mail: gilsonvtorres@hotmail.com
II
Nurse. Master degree in Nursing. Member of the Research Group Incubator of Nursing Procedures. Nursing Department of the Federal University of Rio Grande
do Norte. Natal, Rio Grande do Norte, Brazil. E-mail: liviasemele@hotmail.com
III
Nurse. Doctor in Nursing. Adjunct Professor of the Nursing Department of the Federal University of Rio Grande do Norte. Member of the Research Group Incubator of Nursing Procedures. Natal, Rio Grande do Norte, Brasil. E-mail: isabellekfc@yahoo.com.br
IV
Enfermeira. Doctor in Sociology. Coordinator Professor of the School of Nursing São João de Deus of the University de Évora, Portugal. E-mail: fm@uevora.pt
V
Nurse. Master degree in the Post-graduaton Program in Nursing of the Federal University of Rio Grande do Norte. Scholarship of the Coordenação de
Aperfeiçoamento de Pessoal de Ensino Superior. Member of the Group of Research Incubator of Nursing Procedures. Natal, Rio Grande do Norte, Brazil. E-mail: quinidia@hotmail.com
ABSTRACT
This study compared health-related quality of life (HRQL) domains in people with venous ulcer (VU) treated at the Onofre Lopes University Hospital (HUOL) in Natal, Brazil, and at four primary health care (PHC) clinics in Evora, Portugal. This was a quantitative, analytical, comparative and cross-sectional study of a sample of 130VUpatients. Data were collected from September 2010 to February 2011 using the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36). Respondents scored from5to 95points, averaging48.9points. Comparison revealed significant differences in practically all HRQL domains except pain, as measured by SF-36 in the two countries, and indicated better HRQ Lamong patients treated at the PHC units in Evora than among those receiving care in Natal. To improve HRQL among people with VU requires comprehensive care with multidisciplinary care planning.
Keywords: Nursing; quality of life; venous ulcer; primary health care.
INTRODUCTION
Quality of life (QOL) is a difficult concept, with a view to its subjective, complex and multidimensional character. Having quality of life therefore depends on intrinsic and extrinsic factors. So there is a different connotation of quality of life for each individual, which is caused by the insertion of this in society1.
The correct diagnosis, the adequate treatment and above all the client satisfaction have often been considered as integral factors in the concept of quality of life. So, with some measuring instruments, such as the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), enables the comparison of treatments, allowing the development of strategies in the area of health, with control of effectiveness and maintenance of patients' quality of life2.
The SF-36 has been used in studies on the national scenario3.4 and international5 to evaluate chronic diseases, in particular the venous ulcers (VU), analyzing eight health domains that encompass functional capacity, physical aspects, pain, general health, vitality, social aspects, emotional aspects, mental health and a matter of comparative evaluation between current health conditions and a year ago.
The exchange of clinical trials and the behavioral changes of patients on therapeutic interventions in several places and institutions provide the development and establishment of semi-quantitative measures in evaluating the health profile, thus becoming responsible for the first health status settings6, from there we can see the importance of comparative studies of different strategies of care.
Accordingly, this study aimed to compare the domains of quality of life (QOL) measured by the SF-36 people withVenous Ulcer (VU) attended at the University Hospital Onofre Lopes (HUOL) in Natal/RN, Brazil and four Primary Health Care facilities (PHC) in Évora, Portugal.
LITERATURE REVIEW
The UV is considered a result of inappropriate return of venous blood in the feet or legs, related to various diseases such as: Diabetes Mellitus, peripheral vascular disease, and chronic venous insufficiency (CVI), with approximately 70% to 80% of venous ulcers, are almost exclusively associated with CVI7.
This injury is the most serious complication of CVI, with high prevalence, character polychondritis, which causes suffering to both the patient and his family, in addition to addictiveness of health services, assuming an important magnitude as regards socio-economic repercussions, since it prevents the patient from working, because the injury remains, often open for months or years7-9.
Embora normalmente não fatais, estas feridas crônicas comprometem gravemente a qualidade de vida do paciente devido a mobilidade diminuída e substancial perda de produtividade10.
In Brazil, the VU constitute a serious public health problem, due to the large number of patients with changes in skin integrity, although the records of those calls are scarce, what contributes to encumber the spent in the Unified Health System (SUS), in addition to interfere in the quality of life of the population11.
In Portugal the CVI reaches 2.5 million people, estimated the emergence of about 70,000 new cases per year. A study, including 8243 users of health centers, said a prevalence of 20% in men and 40% in women in the Portuguese population. The estimated prevalence of chronic VU active and inactive was 3.2% in men and 3.9% in women12.
METHODOLOGY
Comparative analytical study with cross-sectional delineation with quantitative approach of processing and data analysis, having as purpose to compare the domains of quality of life measured by the SF-36 people with VU attended in Natal/RN, Brazil and Évora in Portugal.
The locations of the study were the University Hospital Onofre Lopes (HUOL), reference of the Unified Health System (SUS) linked to health complex at the Federal University of Rio Grande do Norte (UFRN), located in Natal/RN, Brazil and four Primary Health Care facilities (PHC), linked to the regional health Board of Évora, members of the National Health System (NHS) of Portugal, being three Family Health Units (FHU) and a Basic Health Unit (BHU) in Évora, Portugal.
The target population of the survey was composed of people with VU attended in these health services in both countries in the period from September to November 2010. Samples for accessibility were composed, by 60 users of outpatient surgical clinic HUOL in Natal/RN, Brazil and 70 users met in PHC in Évora, Portugal.
For selection of people with VU, we had as inclusion criteria: to be the bearer of VU; to be more than 18 years old; to be attended in return consultation or first time in outpatient surgical clinic HUOL in Natal/RN, Brazil and Portugal attended in Évora in selected health units, consent to participate in the survey or having their participation authorized by the responsible with signature of informed consent (TFCC). The exclusion criteria was: request output of the study and have not completed the filling of information of the data collection instruments.
In this research a structured form was used for brief demographic characterization of sample and data collection instrument regarding health-related quality of life (HRQOL) measured by the SF-36.
The SF-36 is a multidimensional questionnaire consisting of 36 items included in eight components: functional capacity (10 items), physical aspects (4 items), pain (2 items), General State of health (5 items), vitality (4 items), social aspects (2 items), emotional aspects (3 items) and mental health (5 items) and a matter of comparative evaluation between current health conditions and a year ago, which is of extreme importance to the knowledge of the patient's disease. This instrument assesses both the negative aspects (disease), as the positive ones (welfare) 12.
The research was approved in both countries, in the Ethics and Research Committee (EPC) of HUOL/UFRN, Brazil, respecting standardization of resolution nº 196/96 as regards the ethical aspects observed when conducting research involving human subjects, no. 279/09 Protocol, and on the Ethics Committee in the area of health and wellfare at the University of Evora in Portugal, Protocol No. 10028/10.
After the agreement of the institutions concerned of the two countries, the data were collected during three months (September to November 2010), and transferred to a database on the application worksheet Microsoft Excel 2007 and after correction, they were exported and analyzed in the program Statistical Package for Social Science (SPSS) version 15.0 Windows.
In the program, SPSS 15.0, descriptive analyses were conducted with absolute and relative frequencies, mean values and standard deviation of scores of variables and inferential analysis at crossings of variables, with statistical significance level of p-value of 0.05, with application < tests-Chi-square χ2 test and T.
RESULTS AND DISCUSSION
For a better overview of the HRQOL comparison of both countries, it is necessary to provide them with an overview of the profile of the sample under study.
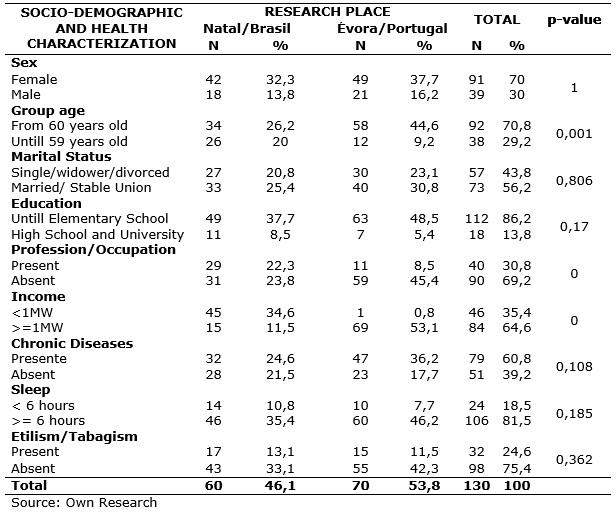
Demographic characterization of VU users surveyed services shows a predominance of female users (70.0%), age range from 60 years old (70.8%), married/stable (56.2%), elementary school (86.2%), income greater than minimum wage (64.6%), absence of profession and occupation (69.2%). As health characterization, 60.8% associated with chronic diseases such as hypertension and diabetes, 81.5% adequate sleep (> 6:0) and 75.4% with absence of alcoholism/smoking, as shown in Table 1.
TABLE 1:
Demographic and health characteristics of users attended in health services of Natal/Brazil and Évora/Portugal, 2011.
Comparing possible differences in the two countries, they are significant in aspects related to age group (p = 0.001) and household income (p = 0.000) and occupation/profession (p = 0.000). These results show that users surveyed in Évora, are older people with better incomes, while having smaller occupation/profession users surveyed in Natal.
The following are the data on health-related quality of life obtained by SF-36 instrument, consisting of 36 items, grouped into eight areas and for each patient with venous ulcer, a score was obtained by applying a measurement scale with values of 0 (worst) to 100 (best state of health).
Analyzing the overall HRQOL score measured by the SF-36 that ranges from 0 (zero) to 100 (one hundred) points, it is seen the overall average of surveyed ranged from 5 to 95 points, averaging 48.9 (dv = 19.2) points, denoting a low quality of life of the surveyed.
When comparing the values of the SF-36 in both countries, it is shown that the surveyed in Natal showed homogeneous variation 29 to 60 points, with an average of 41.8 (dv = 7.8) points which represents low quality, and in Évora a more dispersed variations ranging from 5 to 95 points, while averaging 54.9 (dv = 23.6) showing that the quality of life of the surveyed is better than the surveyed in Natal and this significant difference (p = 0.000) in the T-test for independent samples, as it can be observed in Figure 1.
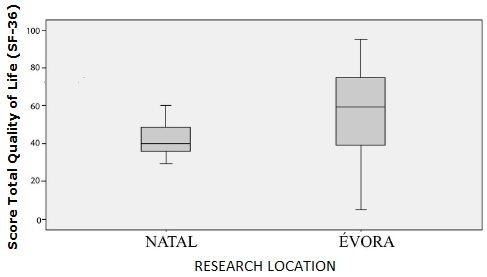
FIGURE 1: Comparison of the total score (T Test, p = 0.000) of the SF-36 according to VU users attended at health services in Natal/Brazil and Évora/Portugal, 2011.
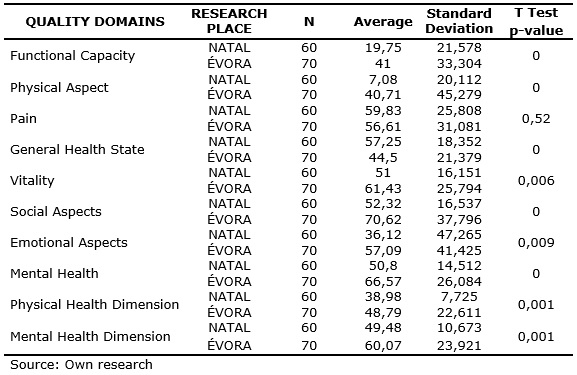
Comparing the HRQOL domains measured by the SF-36, the respondents attended in Évora showed significant differences in relation to the ones attended in Natal in almost all areas such as functional capacity (p = 0.000), physical aspect (p = 0.000), General State of health (p = 0.000), vitality (p = 0.006), social aspects (p = 0.000), emotional aspect (p = 0.009), mental health (p = 0.000), physical dimension (p = 0.001), mental health dimension (p = 0.001), except with regard to pain (p = .520), which highlights the best quality of life of people with VU in this city of Portugal, as shown in table 2.
TABLE 2: Comparison of areas of health-related quality of life according to users with VU attended in health services in Natal/Brazil and Évora/Portugal, 2011.
In searches of several authors, the obtained data corroborate in relation to female predominance, 3: 1 to develop VU, showing a greater tendency of women to develop VU, as reported in some studies13-19.
Patient mobility impaired cause limitations that generate changes in everyday activities that encompass all possible physical aspects, like walking, showering, working, traveling and sleep, routine jobs such as cleaning the house, causing patients to carry out these activities at a slower pace, becoming dependent on others. The physical limitations become major obstacles to keep the wound treatment in a specialized service, due to the difficulty that the patient has on move20.
These data reflect the difficulty that people with Venous Ulcer must dedicate/stay at work and the difficulty in performing these tasks. One of the serious consequences that the venous ulceration brings to the patient is loss of working days, the increase in the number of medical certificate in employment, decreased productivity at work, early retirement and may even lead to unemployment20.21.
The treatment of Venous Ulcer is long and costly, leading to a dependence of the therapeutic behavior. The treatment leads the patients to restrict their daily activities and because of the chronicity of the ulcers take a long period until a cure, which requires commitment and cooperation of patients restrictions22.23. que causa om (2006)7) carreta numa depausa uma grande referidas pelos pesquisados, obtidos a partir do formulizades.
The pain domain is composed of two items, related to pain in the body and the interference of pain at work.
The pain in patients with venous ulcer has been a frequent feature, being worse at night, causing limitation in mobility of the lower limbs affected, disrupting sleep, being described by many patients as a greater impact on their quality of life20.24.25.
A study20 that aimed to describe the problems of the patients with leg ulcers based on etiology or mixed venous insufficiency, in a sample of 141 patients seen in seven hospitals in the Netherlands, the main problems were: pain (85.0%), physical mobility (47.0%) and difficulties in finding appropriate footwear (60.0%).
As for the general state of health, this consists of two items, related to how the researched one regarded his health in a comprehensive way, having others as a reference.
A study on the correlation between clinical classification CEAP and quality of life in chronic venous disease26, was similar to the present study, average of 57.0 with minimum value of 0 and a maximum of 92 in the general state of health for patients with more severe forms of venous disease, namely, those who had ulcers installed.
In the particular case of the studied phenomenon, it is noted that the experience of having chronic venous ulcers may become a source of great suffering for the people who live with this situation. Taking into account the characteristics associated with this change of health, there are: intense pain from the wound, high duration of treatment, the recurring character and chronic instability in the healing process, limitations associated27.
The vitality domain consists of four related items available to the person with the VU in his day to day, his physical strength, his energy, his exhaustion – from the effort caused by the difficulties and limitations of the disease.
A descriptive research to study the experiences of people with chronic VU revealed a set of limitations, a moderate to severe degree, both at physical level as well as at the level of its vitality and daily energy28.
As some studies, the disturbance in sleep pattern is an experience reported by patients with VU, almost always associated with the existence of pain. Fatigue and feeling tired as result of these disorders are conditions that mark regularly presence in the lives of that have a chronic wound and that can have obvious consequences on energy, willingness and ability of people to carry out their normal personal and professional activities29.
Social aspects investigate how VU holders are affected in social activities like visiting friends, relatives, attend events among friends, families. They are composed of two items related to time and so that the injury affected both physically and emotionally that social relationship.
In addition to the obvious physical changes and the enormous financial charges observed, the chronic wounds include also other psychological, emotional and social implications, which is not limited to patients themselves, but which are also extendable to their family and social spheres, reaffirming the complexity of this problem29.
Social aspects in one study30 showed a value of p<0.0001, i.e. extremely significant, and average of 58.1, with standard deviation of 16.3 corroborating this study.
The emotional aspects domain consists of three items – related to changes to the work or any daily activity due to emotional problems – being, among others, the penultimate in relation to the degree of commitment.
In Brazil, a study was developed with the objective of evaluating the quality of life in 30 patients with Chronic Venous Ulcer, also in a public hospital outpatient clinic. The results showed that there was a significant deterioration in the quality of life in some respects, being among them the emotional one31.
The presence of an illness like DVC of same clinical classification might not mean the same for two different individuals, and functional losses resulting from this disease may have emotional and social different amounts for each individual27.
In one study, patients who had the worst scores on the questionnaire SF-36, both in the areas related to physical health how to mental health related, were those who had the most severe form of the venous disease, the ulcer27.
International studies pointed in their results in relation to mental health, feelings of depression, reduction of willpower, helplessness, helplessness, and a sense of impurity. In addition, feelings of guilt, disappointment and sadness in having an ulcer were expressed by the respondents. Continuous frustration has led some patients feel depressed, other patients mentioned feelings of anxiety, social isolation, anger, and decreased self-confidence 26.
The physical dimension comprises the average of the functional domains, physicist, pain, general health and vitality. This analysis allows seeing the relationship of the researched with activities that are influenced by physical aspects and in which the lesion may interfere or not.
The mental health dimension is calculated from the average for the general health, vitality, social function, emotional and mental health aspects. Through this variable, it can be realized the psychological state of the injured, the encouragement and interaction with the environment that surrounds it.
Physical well-being is determined by functional activity, strength, fatigue, sleep, rest, pain and other symptoms; social well-being has to do with the roles and social relationships, the affection and the privacy, the appearance, the entertainment, the isolation, the work, the economic situation and the family suffering; the psychological is related to fear, anxiety, depression and anxiety that cause the disease and treatment. Finally, the spiritual well-being includes the meaning of disease, of hope, of the importance, of uncertainty, of religiosity and internal force32.
CONCLUSION
The total score of the HRQOL measure by SF-36 had below-average value, denoting a low HRQOL of the researched.
However, when compared with the values of the SF-36 in both countries, it was found that those researched in Natal showed homogeneous variation with points below average, which represents low quality, and in Évora a variation more dispersed, although with points above average, showing better and meaningful that the researched in Natal.
When they compared the domains of health related to quality of life as measured by the SF-36 in the two researched countries, significant differences were found in virtually all areas, such as functional capacity, physical appearance, general health state, vitality, social aspects, emotional aspect, mental health, physical health dimension, mental health dimension, except in the area of pain, which highlights the best quality of life of people with VU attended in primary health care services in Évora in relation to the attended in Natal.
The study is limited because it is regional and by requiring follow-up research to identify what factors improve the quality of life of clients during every assistance.
The results of this study can then provide a (re) formulation of new practices of interventions in this area extending the concept of health, allowing focus shift of care centered only on ulcer for a general approach of injury, aiming to interfere with factors that alter the HRQOL of patients and, consequently, improving the care and quality of life of people with ulcers and family.
REFERENCES
1.Rocha SSL, Felli VEA. Qualidade de vida no trabalho docente em enfermagem. Rev Latino-Am Enfermagem [serial on the Internet]. 2004 [citado em 28 fev 2013]; 12(1): 28-35. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692004000100005&lng=en.
2.Castro M, Caiuby AVS, Draibe SA, Canziani MEF. Qualidade de vida de pacientes com insuficiência renal crônica em hemodiálise avaliada através do instrumento genérico SF-36. Rev Assoc Med Bras. [serial on the Internet]. 2003 [citado em 28 fev 2013]; 49(3): 245-9. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-42302003000300025&lng=pt.
3.Silqueira SMF. O questionário genérico SF-36 como instrumento de mensuração da qualidade de vida relacionada a saúde para pacientes hipertensos. [tese de doutorado]. Ribeirão Preto (SP) – Universidade de São Paulo; 2011.
4.Frazão CMFQ, Ramos VP, Lira ALBC. Qualidade de vida de pacientes submetidos a hemodiálise. Rev enferm UERJ [serial on the Internet]. 2011 [citado em 28 fev 2013]; 19(4): 577-82. Available from: http://www.facenf.uerj.br/v19n4/v19n4a12.pdf.
5.Franks PJ, Moffatt CJ. Health related quality of life in patients with venous ulceration: Use of the Nottingham health profile. Quality of Life Research, 2001; 10: 693-700.
6.Ware JE, Gandek B, Iqola Project Group. The SF-36 Health survey: development and use in mental health research and the IQOLA Project. Int J Health. 1994; 23: 49-73.
7.Maffei FHA. Insuficiência venosa crônica: conceito, prevalência, etiopatogenia e fisiopatologia. In: Maffei FHA, Lastória L, Yoshida WB, Rollo HA, Giannini M, Moura R. Doenças vasculares periféricas. 3ª ed. Rio de janeiro: Medsi; 2002.
8.Costa IKF, Melo GSM, Farias TYA, Tourinho FSV, Enders BC, Torres GV et al. Influência da dor na vida diária da pessoa com úlcera venosa: prática baseada em evidências. Rev enferm UFPE on line. 2011; 5(2-spe): 514-21.
9.Brem H, Kirsner RS, Falanga V. Protocol for the successful treatment of venous ulcers. Am J Surg. 2004; 188: 1-8.
10.Leplège A, Hunt S. The problem of quality of life in medicine. JAMA 1997; 278: 47-50.
11.Organização Mundial da Saúde (OMS). Cuidados inovadores para condições crônicas: componentes estruturais de ação: relatório mundial / Organização Mundial da Saúde [serial on the Internet]. Brasília (DF); 2003 [citado em 28 fev 2013]. Available from: http://whqlibdoc.who.int/hq/2002/WHO_NMC_CCH_02.01_por.pdf.
12.Capitão LM, Meneses JD, Oliveira AG. Caracterização epidemiológica da insuficiência venosa crónica em Portugal. Acta Med Port. 1996; 9: 69-77.
13.Sousa FAMR. O corpo que não cura: vivências de pessoas com úlceras venosas de perna. [dissertação de mestrado] Coimbra (Pt): Universidade do Porto; 2009.
14.Costa IKF. Qualidade de vida de pessoas com úlcera venosa: associação dos aspectos sociodemográficos, saúde, assistência e clínicos da lesão Natal, 2011 [dissertação de mestrado]. Natal (RN): Universidade Federal do Rio Grande do Norte; 2011.
15.Silva FAA, Moreira TMM. Características sociodemográficas e clínicas de clientes com úlcera venosa de perna. Rev enferm UERJ, [serial on the Internet] 2011 [citado em 28 fev 2013]; 19(3): 468-72. Available from: http://www.facenf.uerj.br/v19n3/v19n3a22.pdf.
16.Deodato OON, Torres GV. Venous ulcers in users assisted on onofre lopes university hospital, at Natal/RN: sociodemographic and health characterization. The FIEP Bulletin, 2008; 78: 471-4.
17.Vas J, Modesto M, Mendez C, Perea-Milla E, Aguilar I, Carrasco-Lozano JM et al. Effectiveness of acupuncture, special dressings and simple, low-adherence dressings for healing venous leg ulcers in primary healthcare: study protocol for a cluster- randomized open-labeled trial. BMC Complement Altern Med. [serial on the Internet] 2008 [citado em 28 fev 2013]; 8: 29. Available from: http://www.biomedcentral.com/content/pdf/1472-6882-8-29.pdf.
18.Nóbrega WG, Macedo EAB, Dantas DV, Costa IKF, Torres GV. Assessment of the care provided to patients with lower limb vascular ulcers at a university hospital in Natal, Brazil. The FIEP Bulletin, 2008; 78: 350-3.
19.Costa IKF, Nóbrega WG, Costa IKF, Torres GV, Lira ALBC, Tourinho FSV, Enders BC. Pessoas com úlceras venosas: estudo do modo psicossocial do Modelo Adaptativo de Roy. Rev Gaúcha Enferm [serial on the Internet] 2011 [citado em 28 fev 2013]. 32: 561-8. Available from: http://seer.ufrgs.br/RevistaGauchadeEnfermagem/article/view/16715/13940.
20.Heinen MM, Persoon A, Kerkhof PVD, Otero M, Achterberg TV. Ulcer-related problems and health care needs in patients with venous leg ulceration: a descriptive, cross-sectional study. Int J Nurs Stud. 2007; 44(8): 1296-303.
21.Etufugh CN, Phillips TJ. Venous ulcers. Clin Dermatol. 2007; 25: 121-30.
22.Vas J, Modesto M, Mendez C, Perea-Milla E, Aguilar I, Carrasco-Lozano JM, et al. Effectiveness of acupuncture, special dressings and simple, low-adherence dressings for healing venous leg ulcers in primary healthcare: study protocol for a cluster- randomized open-labeled trial. BMC Complement Altern Med. 2008; 8: 29.
23.Hareendran A, Doll H, Wild DJ, Moffatt CJ, Musgrove E, Wheatley C, et al. The venous leg ulcer quality of life (VLU-QoL) questionnaire: development and psychometric validation. Wound Rep Reg. 2007; 15(4): 465-73.
24.Fernandez ML, Broadbent JA, Shooter GK, Malda J, Upton Z. Development of an enhanced proteomic method to detect prognostic and diagnostic markers of healing in chronic wound fluid. Br J Dermatol. 2008; 158: 281-90.
25.Persoon A, Heinen MM, van der Vleuten CJ, de Rooij MJ, van de Kerkhof PC, van Achterberg T. Leg ulcers: a review of their impact on daily life. J Clin Nurs. 2004; 13: 341-54.
26.Moura RMF, Gonçalves GS, Navarro TP, Britto RR, Dias RC. Correlação entre classificação clínica ceap e qualidade de vida na doença venosa crônica. Rev Bras Fisio. [serial on the Internet] 2010 [citado em 28 fev 2013]; 14: 99-105. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-35552010000200003.
27.Beitz J, Goldberg E. The lived experience of having a chronic wound: a phenomenologic study. Dermatol Nurs. 2005; 17: 272-305.
28.Chase SK, Whittemore R, Crosby N, Freney D, Howes P, Phillips TJ. Living with chronic venous leg ulcers: a descriptive study of knowledge and functional health status. J Community Health Nurs 2000; 17(1): 1-13.
29.Santos RFFN, Porfírio GJM, Pitta GBB. Qualidade de vida na doença venosa crônica. J Vasc Bras. 2009; 8(2): 143-7.
30.Longo Junior O, Buzatto SHG, Fontes AO, Miyazaki MCO, Godoy JMP. Qualidade de vida em pacientes com lesões ulceradas crônicas na Insuficiência Venosa de Membros Inferiores. Cir Vasc Angiol, 2002; 17(1): 15-20.
31.Macêdo EAB de, Silva DDN da, Oliveira AKA, Vasconcelos QLDAQ, Costa IKF, Torres GV. Caracterização da assistência prestada à pacientes com úlceras venosas em 10 semanas de uso de terapia convencional. Rev enferm UFPE. 2011; 5: 2129-35.
32.Vinaccia S, Orozco LM. Aspectos psicosociales asociados con la calidad de vida de personas con enfermedades crônicas. Journal Diversitas. 2005; 1(2): 125-7.