RESEARCH ARTICLES
Nursing diagnosis of sexual dysfunction in pregnant women: an accuracy analysis
Cláudia Natássia Silva Assunção QueirozI; Vanessa Emille Carvalho de SousaII; Marcos Venícios de Oliveira LopesIII
IEnfermeira. Graduada em Enfermagem pela Universidade Federal do Ceará, Faculdade de Farmácia, Odontologia e Enfermagem. Departamento de Enfermagem, Fortaleza, Ceará, Brasil. E-mail: c_natassia@hotmail.com
IIEnfermeira. Doutoranda da Universidade Federal do Ceará, Departamento de Enfermagem, Programa de Pós-Graduação em Enfermagem. Fortaleza, Ceará, Brasil. E-mail: v_emille@hotmail.com
IIIEnfermeiro. Doutor em Enfermagem. Professor associado da Universidade Federal do Ceará, Faculdade de Farmácia, Odontologia e Enfermagem, Departamento de Enfermagem.Fortaleza, Ceará, Brasil. E-mail: marcos@ufc.br
ABSTRACT
Across-sectional study with quantitative approach aimed at verifying the accuracy of the indicators of Sexual dysfunction in pregnant women. A questionnaire was applied based on the defining characteristics of North American Nursing Diagnosis Association and the Female Sexual Function Index, applied from July to September 2009. A total of 52 women were selected in a primary health care service in Fortaleza (CE), Brazil to compose the sample. A specialist made the diagnostic inferences. The diagnosis was present in 65.4% and the majority of the defining characteristics were statistically associated. The characteristic perceived limitations imposed by pregnancy was the most sensitive, while alterations in achieving perceived sex role, alterations in achieving sexual satisfaction, changes of interest in others and verbalization of problem were specific. The study results show that is important to verify this diagnosis during the prenatal as the accuracy of the indicators to achieve an accurate diagnosis.
Keywords: Women´s health; nursing diagnoses; sexuality; pregnancy.
INTRODUCTION
At the same time, sexuality is a basic need and a complex phenomenon, which can interfere with physical and mental health of humans1,2. The manifestation of sexuality occurs in various forms, such as a simple look, an expression of affection, a more intimate touch and through emotional intimacy3.
During pregnancy, sexuality undergoes changes ranging from abstinence to increased sexual activity4. These changes lead many couples to believe that this is an improper stage for the sexual act. Thus, the sexualitypattern, established earlier, undergo changes, which may cause constraints and concerns5.
The nursing diagnoses of sexual dysfunction was included in the North American Nursing Diagnosis Association International (NANDA-I) taxonomy in 1980 and revised in 2006. Sexual dysfunction is defined as the state in which an individual experiences a change in sexual function during the sexual response phases of desire, excitation, and/or orgasm, which is viewed as unsatisfying, unrewarding, or inadequate. Its defining characteristics are: alterations in achieving sexual satisfaction, perceived alteration in sexual excitation, alterations in achieving perceived sex role, seeking confirmation of desirability, perceived deficiency of sexual desire, inability to achieve desired satisfaction, perceived limitations imposed by disease, perceived limitations imposed by therapy, actual limitations imposed by disease, actual limitations imposed by therapy, change of interest in others, change of interest in self, and verbalization of problem6.
It is observed that somedefining characteristics of sexual dysfunction are present during pregnancy, being related mainly to changes in the body structure and function, bio psychosocial alterations related to sexuality, conflict of values, erroneous or lacking knowledge and vulnerability, among others6. However, the association between pregnancy and sexual dysfunction has been little investigated.
It is considered that studies of defining characteristics’ accuracy contribute to the development of a greater diagnostic certainty, and may reflect the improvement inthe quality of nursing care.
Therefore, we developed this study in order to verify the accuracy of the clinical indicators of sexual dysfunction in pregnant women.
THEORETICAL REFERENTIAL
The identification of nursing diagnoses should be grounded on evidence, therefore, the use of good clinical indicators is crucial. The importance attributed by nurses, to a specific indicator or to a set of indicators determines the accuracy of the diagnostic inference and influence the care plan. Accurate clinical indicators are those that contribute to validate a nursing diagnosis in the clinical setting7.
At this point, a valid, reliable and stable nursing diagnosis is one that corresponds to the actual state of the measured phenomena, which is essential for the development of an effectiveand individualizedcare plan8.
Given that the analysis of human responses is the basis ofnursing care, the continuing development of critical thinking skills is necessary. It is emphasized that an accurate diagnosis is essential to help the patient, but the process of identifying the best or most accurate diagnoses is challenging due to the complexity of human beings9,10.
One way to verify the accuracy of clinical indicators is the calculation of accuracy measures, such as sensitivity, specificity and predictive values. Sensitivity is defined as the proportion of people with certain diagnosis, which presents a clinical indicator. Specificity refers to the proportion of individuals without the diagnosis, which don’t presents a certain clinical indicator. The positive predictive value indicates the probability of the presence of the diagnosis when a clinical indicator is present, while the negative predictive value is the probability of the non-occurrence of the diagnosis when a particular clinical indicator is absent11.
For many clinicians, accuracy should be the main objective of the diagnostic process, because the collected inferences are based on clinicaljudgment and probabilities, so, there is always the risk of error7. Therefore, it is necessary to develop research in nursing diagnoses addressing the accuracy of clinical indicators.
METHODOLOGY
This cross-sectional study was carried out with pregnant women in a primary health care service of the city of Fortaleza (CE), Brazil. This service provides prenatal and gynecological preventing consultations conducted by nurses to women from the area attached to the service. The research consisted in the collection of socio demographic and clinical data of pregnant women and in the identifications ofsexual dysfunction.
The sample was composed by pregnant women that received medical care at the institution, and which maintained an active sex life after the onset of pregnancy. The presence of diseases that could influence the profile of the defining characteristics of sexual dysfunction was considered as an exclusion criteria. The sample size was calculated through the formula for finite population, resulting in a number of 52 women that were selected by convenience sampling, as they were seeking the service.
The approval for the study was granted after the clarification of the research objectives by signing the Informed Consent. The ethical research principles were respected and the study was approved by the Ethics Committee responsible for research, under the protocol 166/09.
Data collection was conducted through interviews in a private room, in the period from July to September 2009. We used an form developed based on NANDA-I6 and on the Female Sexual Function Index (FSFI)12, a brief scale designed to assess sexual function in women, which has submitted acceptable statistical validity13.
The form contained identification data, obstetric data and questions concerning the defining characteristics of sexual dysfunction, based on a model of diagnostic validitycontent14.
Data collection results were analyzed by a master in nursingthat is specialized on diagnostic inferences. The decision to consult this specialist occurred because she have defended dissertations and recent published articles involving the use of NANDA-I taxonomy. The following Gordon diagnostic reasoning steps were used: assessment, information grouping and definition of diagnostic categories15.
Data were analyzed using the program Predictive Analytics SoftWare (PASW) version 18.0. Demographic, socio obstetric data and responses related to the defining characteristics of sexual dysfunction were defined as independent variables, while sexual dysfunction was defined as the outcome. The results were presented in tables and the Kolmogorov-Smirnov test was used to verify the normality.
For descriptive and inferential analysis, the Chi-square test (association between variables) and the Fisher test (for expected frequencies less than five), with significance set at p<0.05 were used. The magnitude of the association was calculated through the prevalence ratio test. Sensitivity, specificity, positive and negative predictive values were obtained for the accuracy analysis. A cutoff point of 80% was defined, above which the results were considered relevant.
RESULTS AND DISCUSSION
Of the 208 pregnant women enrolled in the study, 52 were selected. Of these, 38 (73.1%) were unemployed and 15 (28.8%) had studied until high school. The monthly family income of 25 (48.1%) respondents was below the minimum wage (equivalent to R$ 465.00).
The high prevalence of unemployment can be related to limitations related to pregnancy as to the age of most of the interviewees. Studies shows that the division of labor and power between men and womenthroughout the development of societies is a cultural invention, and that the forms of social labor division excludes and discriminate women recurrently16.
The interviewees were aged between 14 and 39 years, with a mean of 22.38 years (± 5.057) and the number of pregnant adolescents was 16 (30.77%).
Statistics shows that 19.3% of Brazilian women are teenagers, less than the number found in the present study sample17. Sexual dysfunction was found in 34(65.4%) case, 15 (29.4%) corresponding to teenagers, a result that draws attention, considering that, often, the healthcare team is not willing to listen, discuss and guide this population regarding sexuality, which creates uncertainty and undermines the sexual performance18.
The gestation period is, for some teens, the ultimate expression of femininity, which confirms the sexual identity. Thus, self-esteem rises enough that, in many cases, these women face the emotional difficulties of pregnancy and being able to reconcile the exercise of sexuality in the obstetrical condition5. Given this premise, it can be inferred that sexuality must be addressed by nurses during the prenatal care, regardless of the woman’sage.
In relation to pregnancy, 20 (38.5%) women were in the 3rd trimester of pregnancy. Of the total, 33 (63.5%) stated that the pregnancy was unplanned. The average uterine height was 25.7 cm and 27 (51.92%) women attended at least two prenatal consultations (median). The number of primiparous was 27 (51.92%) and the average number of abortions was less than one.
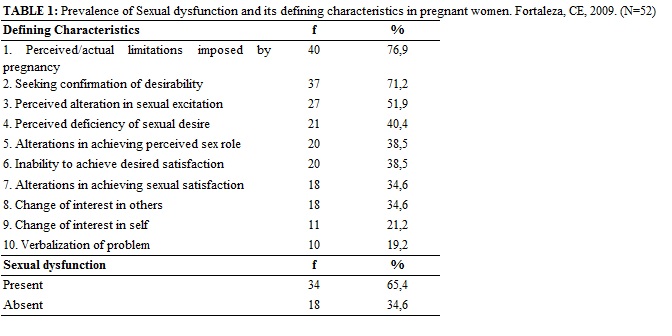
The frequency of sexual dysfunction was 34 (65.4%). The defining characteristics more present, i.e., with frequency greater than 40% were: perceived/actual limitations imposed by pregnancy - 40 (76.9%), seeking confirmation of desirability - 37 (71.2%), perceived alteration in sexual excitation – 27 (51.9%), and perceived deficiency of sexual desire - 21 (40,4%),as shown in Table 1.
The perceived/actual limitations imposed by pregnancy shall be understood as physical or psychological restrictions that may interfere with sexual response phases, whether or not concomitant. The actual limitations can be proven and clinically observed and result in the presence of a particular condition. Moreover, limitations are related to perceived limitations experienced by individuals19.
The defining characteristic perceived/actual limitations imposed by pregnancy has been identified in 40 (74.9%) women who had at least one of the following manifestations: abdomen increase, dyspareunia and decreased lubrication. The literature suggests a negative self-image as a common symptom in pregnancy, and that the increased volume of the breasts and abdomen, exacerbated weight gain and other changes common to pregnancy sometimes had an anti-erotic effect. The modified perception about oneself and the lack of knowledge about what happens physically and emotionally leads to insecurity, affecting sexual performance5.
It is noteworthy that, in some cases, certain defining characteristics were present, however, the expert did not consider the diagnosis as present. This is due to the fact that the diagnostic conclusion is made based on a set of defining characteristics and not based just on isolated indicators. For further investigation, we proceeded to analyze the association between sexual dysfunction and each defining characteristic.
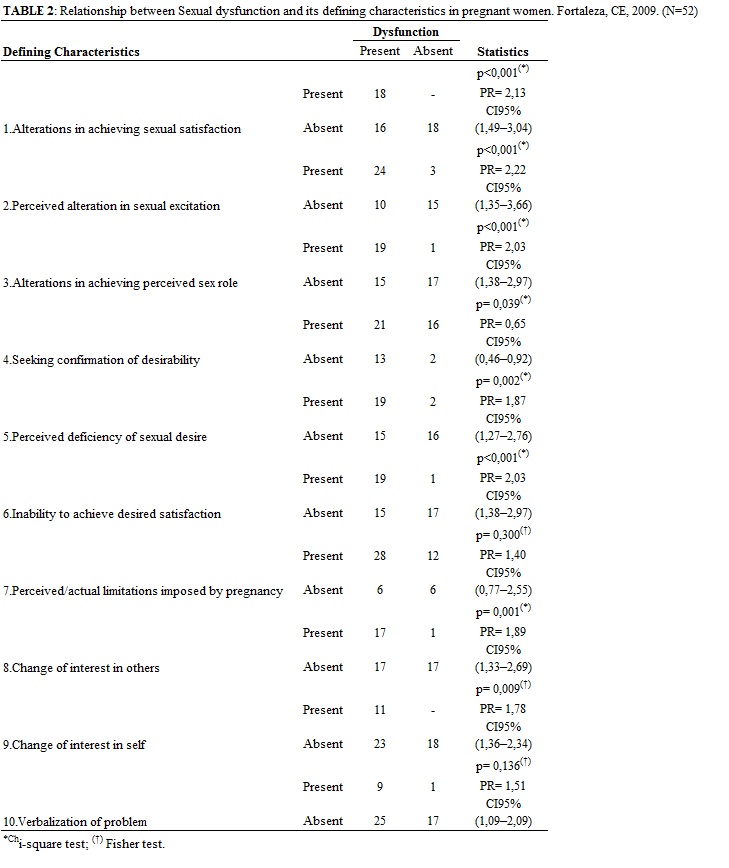
Considering the level of statistical significance (p <0.05), except for perceived/actual limitations imposed by pregnancy and verbalization of problem, all defining characteristics were significantly related to the nursing diagnosis, as shown in Table 2.
The defining characteristic seeking confirmation of desirability was the only one with confidence interval less than one(0.46 to 0.92), indicating that the presence of this defining characteristic seems to act as a protective factor for sexual dysfunction. It was also emphasized that the defining characteristics alterations in achieving sexual satisfaction, perceived alteration in sexual excitation, alterations in achieving perceived sex role, and inability to achieve desired satisfactionstood out with the highest values of prevalence ratio ( PR> 2).
The defining characteristicseeking confirmation of desirability addresses the change in sexual desire, in the sense of not feeling desirable or failing to arouse sexual desire in others, which can result in sexual disinterest.
We know that having a positive body image is essential, as this will strengthen in women, especially pregnant, sense of attractiveness, social acceptance, and ability to give and receive affection, the way we perceive ourself and, especially,ability to establish and maintain loving ties18. The inverse correlation is justifiable because, once the sexual dysfunction is installed, probably the interested in confirming the quality of being desirable will disappear or it will ceases to be a focus of concern for the women.
Alterations in achieving sexual satisfaction, perceived alteration in sexual excitation, alterations in achieving perceived sex role, and inability to achieve desired satisfactionexhibited the highest prevalence ratio. These findings are justified, given that each of these defining characteristics are expressed manifestations of sexual dysfunction.
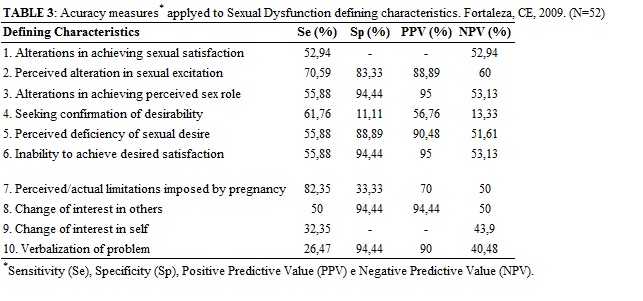
The accuracy analysis pointed that perceived/actual limitations imposed by pregnancy was the defining characteristic with higher sensitivity(82.35%). The defining characteristics alterations in achieving perceived sex role, alterations in achieving sexual satisfaction, change of interest in others, and verbalization of problem had a high specificity value (94.44%), according to Table 3. The defining characteristics alterations in achieving perceived sex role (95%) and alterations in achieving sexual satisfaction(95%) had high positive predictive value, i.e., greater than 94.9%. No characteristic showed a high negative predictive value, i.e., greater than 80%.
Sexual intercourse is avoided by women during pregnancy, most often, for fear of pain, as found in 21 (40.39%) women in this study. A study points that sexual disposition of most women decreases during pregnancy20, but in some cases sexual activity is maintained with a different pattern compared to non-pregnant4,5.
The difficulties in performance and sexual satisfaction of women affect the quality of life21. The inability to achieve desired satisfaction and the alterations in achieving sexual satisfactionareindicators that cover sexual satisfaction of three phases of sexual response, especially in relation to the phase of orgasm since it is characterized by feelings of pleasure. In this study, this difficulty was pointed out by 18 (34.6%) women.
Another important point is the presence of the defining characteristic verbalization of the problem, that showed a low prevalence 9 (19.2%) and high specificity (E = 94.44). One clinical indicator is considered specific when its absence is related with the absence of the nursing diagnosis22. This finding may be related to the fact that many women find it difficult to discuss the changes in sexual functionopenly.
The findings reinforce the importance of reflection, by nurses, about the mechanisms that generate values and attitudes regarding sexuality. We emphasize that the approach of the sexuality during prenatal consultation is still deficient. Often, the nurses focuses only pregnancy issues, neglecting issues such as the relationship between the woman and her own body, sexuality and relationship problems23.
CONCLUSION
This study enabled us to determine the prevalence of sexual dysfunction in pregnant women and to measure the accuracy of the defining characteristics of this diagnosis.Different values of sensitivity and specificity to the analyzedvariables were obtained.
The possibility of the occurrence of an imperfect gold standard represents a limitation of the study as in any research involving diagnostic inferences. The imperfect gold standard relates to the fact the presence/absence of a nursing diagnosis is inferred based on a personal point of view of an individual (a specialist on nursing diagnoses). We tried to minimize this effect by using the consensus of members of a research group when the consulted specialist had doubts about the diagnostic conclusion.
Moreover, the lack of studies focused on the accuracy of the defining characteristics and nursing diagnoses, especially on the Sexuality domain, limited the discussion of the findings.
The results have implications for the practice of prenatal nurses, because it is necessary to recognize the changes in female sexual pattern resulting from pregnancy, which relates not only to how sexuality is experienced, but also in how those changes affect other aspects of life. Nurses must respect the peculiarities of each patient, identifying and individualizing responses to health alterations pertaining to sexuality.
REFERENCES
1. Alden KR, Lowdermilk DL, Cashion MC, Perry SE. Maternity and Women's Health Care. St Louis (USA): Mosby; 2011.
2. Martins CBG, Alencastro LCS, Mato KF, Almeida FM, Souza SPS, Nascimento SCF. Gender issues regarding adolescent sexuality. Rev enferm UERJ. 2012; 20:98-104.
3. Nezhad MZ, Goodarzi AM. Sexuality, intimacy, and marital satisfaction in Iranian first-time parents. J Sex Marital Ther. 2011; 37(2):77-88.
4. Camacho KG, Vargens OMC, Progianti JM. Adapting to the new reality: the pregnant woman and the exercise of her sexuality. Rev enferm UERJ. 2010; 18:32-7.
5. Araújo NM, Salim NR, Gualda DMR, Silva LCFP. Body and sexuality during pregnancy. Rev esc enferm USP. 2012; 46(3):552-8.
6. Herdman, TH. NANDA international nursing diagnoses: definition& classification, 2009-2011. Hoboken (USA): Wiley-Blackwell; 2009.
7. Lopes MVO, Silva VM, Araujo TL. Methods for establishing the accuracy of clinical indicators in predicting Nursing Diagnoses. Int J NursKnowl. 2012; 23:134-9.
8. Oliveira ARS, Costa AGS, Moreira RP, Cavalcante TF, Araujo TL. Nursing diagnoses in the activity/exercise class with stroke patients. Rev enferm UERJ. 2012; 20: 221-8.
9. Mata LRF, Souza CC, Chianca TCM, Carvalho EC. Creating diagnoses and interventions under the auspices of different nursing classification systems. Rev esc enferm USP. 2012; 46:1512-8.
10. Minthorn C, Lunney M. Participant action research with bedside nurses to identify NANDA-International, Nursing Interventions Classification, and Nursing Outcomes Classification categories for hospitalized persons with diabetes. ApplNurs Res 2012; 25:75-80.
11. Fletcher RH, Fletcher SW, Fletcher GS. Clinical epidemiology: the essentials. Philadelphia (USA): Lippincott Williams & Wilkins; 2012.
12. Rosen RC, Brown C, Heiman J, Leiblum S, Meston CM, Shabsigh R, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000; 2:191-208.
13. Baser RE, Li Y, Carter J. Psychometric validation of the Female Sexual Function Index (FSFI) in cancer survivors. Cancer. 2012; 118:4606-18.
14. Fehring RJ. The Fehring model. In: Carrol-Johnson RM, Paquete M. Classification of nursing diagnoses: proceedings of the Tenth Conference. Philadelphia (USA): JB Lippincott; 1994. P. 52-62.
15. Gordon M. Manual of nursing diagnosis. Greater Sudbury (USA): Jones and Bartlett Publishers; 2009.
16. Alves AES. Sexual division of labor: separating production from the family's reproductive space. Trabeducsaúde. 2013; 11:271-89.
17. Brazilian Ministery of Health (Br). Secretaria de VigilânciaemSaúde. SaúdeBrasil 2011: umaanálise da situação de saúde e a vigilância da saúde da mulher. Brasília (DF): Brazilian Ministery of Health; 2012.
18. Albuquerque JG, Pinheiro PNDC, Lopes MVO, Machado MDFAS. Knowledge deficit regarding HIV/AIDS in adolescent students: identifying the NANDA nursing diagnosis. Rev EletrônicaEnferm. 2012; 14:104-11.
19. Ferreira DQ, Nakamura MU, Souza ED, MarianiNeto C, Ribeiro MC, Santana TDGM, et al. Sexual function and quality of life of low-risk pregnant women. Rev Bras Ginecol Obstet. 2012; 34:409-13.
20. Sanfelice C, Carbonell CS, Antunes LW, Neumaier CA, Nunes CB, Ressel LB. Knowledge and care practices of pregnants of a basic health unit. Rev Enferm UFPE. 2013; 7(12):6790-9.
21. Liebergall‐Wischnitzer M, Paltiel O, Hochner DC, Lavy Y, Manor O, Woloski ACW. Sexual function and quality of life of women with stress urinary incontinence: a randomized controlled trial comparing the Paula method (circular muscle exercises) to pelvic floor muscle training (PFMT) exercises. J Sex Med. 2012; 9:1613-23.
22. Katz DL, Wild D, Elmore JG, Lucan SC. Epidemiology, biostatistics, preventive medicine, and public health 4th ed. Philadelphia (USA): Saunders; 2013.
23. Costa LHR, Almeida ECC. Nursing and sexuality: integrative review of papers published by the Latin-American Journal of Nursing and Brazilian Journal of Nursing. Rev Latino-Am Enfermagem. 2011; 19:631-9.
Recebido em: 12.06.2012
Aprovado em: 08.10.2013