RESEARCH ARTICLES
Nursing consultation: evaluation of adherence to self-care in patients undergoing radiotherapy
Karla Biancha Silva de AndradeI; Anna Clara Lima FranczII; Marianne dos SantosGrellmannIII; Priscila Cortez BelchiorIV; Josiana Araujo de OliveiraV; Dayse do Nascimento WassitaVI
INurse. PhD in Nursing. Associate Professor, Graduate School of Nursing at the State University of Rio de Janeiro. Nurse of the National Cancer Institute. Brasil. E-mail: k.biancha@ig.com.br
IINurse. Graduated from the State University of Rio de Janeiro. Brasil. E-mail: annafrancz@yahoo.com.br
IIINurse. Postgraduate in Oncology by Federal University Fluminense. Rio de Janeiro, Brasil. E-mail: mari.grell@hotmail.com
IVNurse. Graduated from the State University of Rio de Janeiro. Brasil. E-mail: pribelchior@hotmail.com
VNurse. Masters in Nursing Student by the State University of Rio de Janeiro. Postgraduate in Critical Care (Residency). Substitute Professor at the Faculty of Nursing at the State University of Rio de Janeiro. Brasil. E-mail: josianaoliveira@yahoo.com.br
VINurse. Specialist in Oncology Nursing by the National Cancer Institute. Chief of Nursing Service of Radiotherapy, University Hospital Pedro Ernesto. State University of Rio de Janeiro. Brasil. E-mail: dede2381@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2014.11227
ABSTRACT
This study aimed to assess patient adherence to the guidelines provided in nursing consultation in radiotherapy. This is a descriptive study with a quantitative approach, performed in a University Center for Cancer Control in the State of Rio de Janeiro. 37 patients undergoing radiotherapy were assessed through questionnaires containing 16 items related to the profile and patients' adherence to oriented care, applied in May 2012 The results showed that the majority of respondents were male (62%), with predominant age group of 58-67 years old (38%), the majority treated tumors in the head and neck (51%), 90% reported adhering to the guidelines of self-care and 54% did not develop radiodermatitis. It was concluded that the nursing consultation is important in care to patients undergoing radiotherapy and may influence treatment adherence and to clarify doubts about the therapeutic plan.
Keywords: Nursing Consultation; Radiotherapy; Self-care; Adhesion.
INTRODUCTION
Cancer is a chronic disease and is an ongoing public health problem worldwide. Each year, the number of diagnosed cases grows. For 2014 and 2015, the National Cancer Institute (NCI) estimates the occurrence of approximately 576,000 new cases of cancer in Brazil, reinforcing the magnitude of the problem¹.
Given these data, it is opportune to develop strategies for prevention and control of disease, access to diagnosis and treatment in a timely manner, as well as a safe care that minimizes undesirable effects from the treatment plan.
Among the treatments for cancer, radiation therapy is used on a large scale and can have curative or palliative purpose, in terms of tele therapy and brachytherapy. However, despite its desired results, individuals in contact with radiation may develop manifestations of toxicity such as mucositis and radiodermatitis2,3. The initial skin reactions after radiotherapy are generally moderate, but more than 90% of patients treated with radiotherapy develop skin reactions2.
Thus, preventive measures must be developed in order to minimize acute radiotoxicity during treatment. Nursing consultation becomes critical at this time, being an essential tool for the quality of life of patients and a favorable condition to offer a secure care4.
The protocol of the NCI systematizes the guidelines given during the nursing consultation through a self-care guide to the irradiated skin to minimize the damage caused by radiation used during treatment, even considering its limitation to prevent the development of such reactions5,6.
Among the self-care guidelines in this protocol and performed by the nurse we can cite: Use moisturizing cream based on aloe vera, avoid water jet directly on the irradiated skin and hair removal with razor or wax, encourage the intake of two liters of fluid a day and recommend not exposing the skin to sunlight during treatment5,6.
Such guidelines should comprise the treatment plan, which should also stress the importance of attending medical appointments, changes in lifestyle during treatment and clarifying questions as they arise during this period. In this regard it is worth questioning whether the nursing consultation can help in minimizing complications related to radiotherapy in cancer patients undergoing treatment.
Nursing consultation elucidates common and isolated doubts of patients initiating therapy process, establishing itself as an appropriate moment for better understanding by the patient about the disease and the importance of adhering to the radiotherapy sessions4-7. Thus the present study aimed to assess patient adherence to instructions given in the nursing consultation in radiotherapy.
LITERATURE REVIEW
Radiotherapy uses ionizing radiation, which has energy enough to ionize molecules by releasing electrons from atomic structure, such as X-rays alpha and beta particles. Radioisotopes are used in high doses, precisely targeting the deleterious effect of radioactivity on certain tissues, aiming to achieve a favorable therapeutic index and causing malignant cells to lose their clonogenicity2,7.
The skin is an organ characterized by having cells with rapid cell division cycle, an important factor in radiosensitivity, and, therefore, it is the first to manifest adverse tissue reactions to ionizing radiation5. Thus, the radiodermatitis are skin lesions considered adverse events and may involve approximately 95% of patients treated with radiotherapy. The most common reactions are: dry skin, pruritus and erythema after three weeks of completion of radiation2,5,8.
The protocol of the NCI has been widely used by hospitals and oncology services in order to maximize the effectiveness of preventive actions5-7. This protocol also recommends assessment of parameters of tumor location, of doses and specific energy that interfere with the acute toxicity of the skin and oral mucosa, and the guidance of self-care practices, with the goal of preventing complications and/or minimize the inevitable side effects2,5,8.
According to Resolution No. COFEN 159/1993, nursing consultation is a private activity of the nurse and uses components of the scientific method to identify situations of health/illness, to prescribe and implement nursing actions that contribute to health promotion, protection and prevention of injuries, recovery and rehabilitation of the individual, family and community9.
In addition, Resolution No. COFEN 211/1998 regulates the activities of nursing professionals in Radiotherapy, Nuclear Medicine and Imaging services10. In accordance with these resolutions, the nurse should participate in therapeutic nursing protocols, promote and disseminate preventive and curative health measures, utilizing the nursing consultation to formulate and implement explanatory manuals through education to patients and families, adapting them to their social realities5-7,10.
METODHOLOGY
This is a descriptive study with a quantitative approach based on the selected object. A descriptive study aims to study the characteristics of a group, survey of opinions, attitudes, beliefs of a population or the identification of relationships between variables11,12.
The research was conducted at the University Center for Cancer Control, reference service in radiotherapy of a university hospital located in the municipality of Rio de Janeiro. Such service includes the Teacher Assistance Unit – TAU of Radiotherapy, the Palliative Care Clinic and part of the Department of Radiology and Diagnostic Imaging. According to information provided by the unit, is serves a monthly average of 50 patients.
We analyzed patients undergoing radiotherapy treatment for two groups of specialties: cancer of the head and neck, breast, female pelvis, male pelvis, and thorax and abdomen, which underwent four and three nursing visits, respectively, at different moments that guide this treatment.
The data collection instrument was a questionnaire formulated with 16 closed questions divided into two parts: the first part, with five questions about the patient profile including sociodemographic variables (age, sex, education and income); and the second part with 11 questions about their adhesion on the oriented care during the nursing consultation, containing the variables: development of radiodermatitis, adherence to self-care to prevent radiodermatitis and location of the tumor.
Five items related to the care that must be performed were listed: general skin care, the use of aloe vera moisturizing, the maintenance of nails trimmed and clean, the intake of two liters of water per day and the use of chamomile tea in the skin. Also, five items on actions that should be avoided were considered: the force of the water jet in the skin, the use of razor or wax, the use of dark and synthetic materials clothing, the exposure of the skin to the sun and the physical effort.
The criteria for inclusion of subjects in the study were: consent for participation, be literate, have over 18 years old and be scheduled for the penultimate or last nursing consultation on the questionnaire. The last criterion was justified by the increased possibility of patient presents adverse effects to radiotherapy and the longest period of relationship between nurse-patient. The exclusion criteria were: illiteracy, pain at the time of the interview and having hearing, visual and/or motor disability.
The project was submitted to the Research Ethics Committee 13 of Sub-Dean of Graduate Studies and Research at the State University of Rio de Janeiro and approved under the number 006.3.2012. Data collection occurred in May 2012, being initiated only after the approval of the Head of the unit and the signing of free and informed consent form by patients.
Data were tabulated and analyzed using simple frequency. The obtained information generated a database, which based the creation of tables and graphs, using MS-Excel version 2007 software.
RESULTS AND DISCUSSION
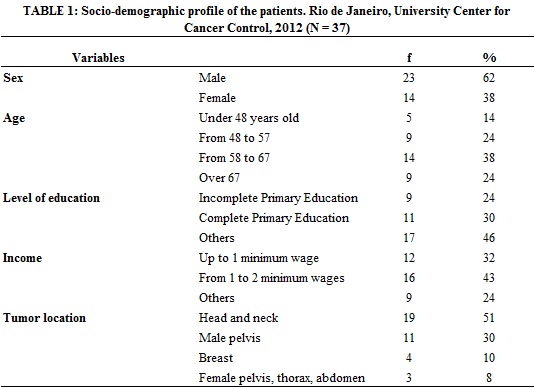
The study included 37 individuals. The analysis of socio-demographic information showed that in this group, 22 (62%) are male; that prevalent age group was 58-67 years old, with 14 (38%) participants; 16 (43%) receive one to two minimum wages, followed by 12 (32%) receiving up to one minimum wage. A third of the participants have completed elementary education (11), followed by 9 (24%) who had not completed elementary education, as shown in Table 1.
The results differ from the literature on the prevalence of cancer according to sex, because national statistics indicate that there is no significant difference in the prevalence and incidence between the sexes. Differences occur primarily by tumor location and lethality of each type of cancer. The predominant age groups found have a close relationship with tumor locations of participants, such as breast, head and neck and prostate1,14.
The level of education is associated with greater knowledge about cancer, and a higher income can influence the history of the pathology of the patient, since cancer is more prevalent among groups of larger social exclusion, as they undergo major risk factors of illness and death1,14,15.
Thus, there is a relationship between income and tumor location linked to lifestyle habits such as mouth cancer and uterine cervix, more frequent among young adults with low income and education14,15.
Regarding the location of the tumor, 19 (51%) treated tumors located in the head and neck, followed by 11 (30%) tumor located on the male pelvis and 4 (11%) breast cancer.
Tumors that make up the list head and neck, such as the larynx and esophagus, have a major impact on the population, but do not exceed the occurrence of breast and prostate cancer for example. Prostate cancer, pathology of the male pelvis, was considered the second most common type of cancer in men. Since breast cancer is the type of cancer that affects more women around the world, both in developing countries as in developed countries1,14,15.
Evaluation of adherence to self-care guidance provided during nursing consultations showed that 33 (90%) participants reported having adhered to the recommendations and 20 (54%) participants reported that they had not developed radiodermatitis during radiotherapy treatment.
It is observed that the use of radiotherapy for cancer treatment has proved to be an effective adjuvant in tumor regression15,16. Despite advances, adverse effects are still observed during and after radiation treatment. One of the most common effects are acute skin reactions, which can range from a mild erythema and itching to tissue necrosis, through dry or moist desquamation2-4,6-8.
In this sense, preventive measures need to be prescribed during the Nursing consultation, in order to reduce the radiotoxicity2,4-6,8,17,18.
The distribution of care adopted by customers is described in Table 2.
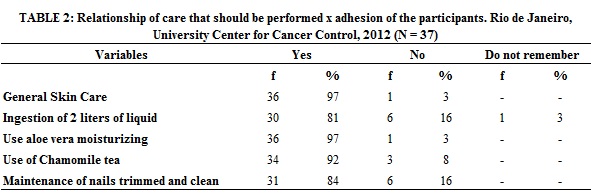
In relation to skin care, 36 (97%) reported they have had such care in the irradiated region, 30 (81%) reported having consumed two liters of liquid per day during treatment, 36 (97%) used the aloe vera ecossoma moisturizer, 34 (92%) made use of chamomile tea to soothe irritative effects on the skin. Furthermore, it was evident that most chose to keep the nails trimmed and clean, making 31 (84%) of the participants.
The basal water requirement for adult dependends of sensitive losses of water (urine) and insensitive lossos of water, and varies 1250-3000 ml/day, depending on the body surface, cell number, age, weight and sex. Moreover, it should be considered clinical states of loss or retention. Thus, it is necessary stimulus for monitoring fluid intake, aiming at the adequate hydration for efficacy and decreased toxicity during treatment17,19.
Although most patients stated intake of 2 liters of fluid per day, five (16%) did not have this practice and one (3%) did not remember if it proceeded. This information instrumentalizes the nurse that during nursing consultations, give greater emphasis as fluid intake, which should be a common habit to any individual, regardless of their pathology19,20.
On the unit on which the survey was conducted, the aloe vera ecossoma moisturizing is offered, which should be used after radiotherapy session, as well as the moisturizing soap which should be used to wash the irradiated region. Thus, in this study we observed greater adherence related to the use of these materials, since they are delivered from the first consultation care.
Given the observed effectiveness of preventive care, various sevices adopted products or curatives that applied in the irradiated area, intended to prevent the increase of the degree of radiodermatitis, reducing patient discomfort and downtime of radiotherapy. This topical treatment implies compress of water and chamomile tea, essential fatty acids lotion-based (EFA) and aloe vera to soften the effects of radiation on the skin2,4-6,20,21.
Despite the deficiency of scientific studies proving the efficacy of the use of chamomile plants, units for treatment of oncology have observed good results, helping to reduce damage and moisturizing the skin, thanks to its emollient effect6,20,21. In this study, we found that adherence to herbal method was high (92% use chamomile tea), either by the low cost, or by the patients’ beliefs and values, or even by the effectiveness that this method presents.
Another very important care is to maintain the nails cleaned and trimmed, which prevents skin damage and itching at the place of infection, since when patient to scratchs it, it can favor the radiodermatitis, since cancer patients suffer from immunosuppression and skin sensitivity due to radiotherapy5,6,8,17,18.
In nursing consultations, besides guidelines for the care of the irradiated region, preventing the emergence of radiodermatitis, guidelines for actions that should be avoided during treatment are also provided. It was found that 32 (84%) of patients report maintaining these crucial care, as shown in Table 3, that describes the relationship between the actions that must be avoided to anticipate complications with the corresponding adhesion of the participants.
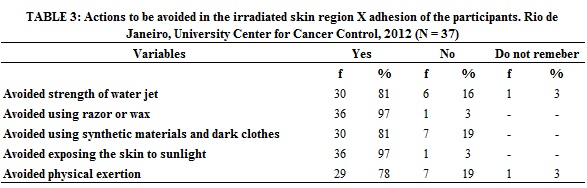
On this research, 29 (78%) reported avoiding physical exertion. Fatigue is the most common symptom experienced by cancer patients and their careful measurement and evaluation are critical to assess the effectiveness of intervention strategies with the patient and his family. Fatigue is defined as a multidimensional, multi-causal sensation and similar in its complexity to pain. So it becomes essential to avoid physical exertion during treatment, guiding the choice for rest and relaxation17,21.
Besides fatigue, malaise and anorexia are also checked. These symptoms may be secondary to substances released when tumor cells are cleaved. The effects are temporary and decrease with treatment interruption18,22,23.
Regarding to avoid jets of water and avoid using dark clothes and synthetic material, 30 (81%) participants reported adhering to such preventive measures as well as 35 (97%) avoided the use of razors or wax and sun exposure. Such care favor the maintenance of skin integrity by not causing friction, scratching or trauma4,6,8,17,18,20.
Although the results of the research have shown a high degree of adherence to preventive guidelines, it was observed that a significant index of radiodermatitis still prevailed. This led to reflect on some assumptions, especially regarding the confirmation of adherence to the proposed preventative treatment. Because it cannot be said that the patient correctly follows the guidelines provided only through the their answers, since patients may feel afraid to reveal non-compliance with them, mainly because they have been oriented during the consultation24,25.
The nursing consultation to patients and to those who are involved with their disease, should consider the life history of each individual, the impact of the disease and its treatment in their reality. Thus, the care plan should take into consideration, among other aspects, the social reality of the subjects in this condition4,6,7,9,23-25.
Another assumption is the fear that, if they answer something that is not within what was oriented, they can be treated differently, even if the failure is due to some personal difficulty, involving financial resources, for example.
In this context, helping the patient understand the process in which he appears is to make him able to face this moment of his life, supporting the potential complications. More effective communication between staff and the patient may improve adherence to treatment and care to be implemented, as well as, help to minimize the risks of therapeutic strategy4,6,24-26.
CONCLUSION
The research results provided an overview of the consultation carried out in nursing radiotherapy unit with a view to compliance with protocols established by the Ministry of Health, following a standard of quality which can directly influence adherence to self-care.
It is important that the patient understands the principles of each treatment and how they relate to each other. This enables understanding of the objectives of the treatment plan for improving the quality of life of individuals with oncological disease.
The nurse must consider the patient as a whole, considering the socioeconomic aspect since such aspects may influence their adherence to self-care during treatment.
In relation to radiotherapy, the development of radiodermatitis is an expected adverse complication due to toxicity conferred by radiation. Although most participants claimed to have adhered to the guidelines, the incidence of radiodermatitis was still high. In addition to this, tumor location in the head and neck, being one of the most sensitive regions to radiation, leads naturally to higher prevalence of these lesions.
So, the nursing staff, specifically the nurse should provide a favorable environment for guiding prevention actions and solving relevant questions.
The research addressed issues that pervade by some aspects in relation to adherence to guidelines given during nursing consultations. These aspects permeated from patient involvement with treatment until the understanding about the real necessity of self-care practices to reduce the inherent damage of the therapeutic plan. It was understood that in order to develop a plan of care to patients in the radiotherapy department, it is necessary that the nurse take into account how the patients and their caregivers are experiencing the phenomenon of being sick. For this, integration between patients, caregivers and nurses is necessary.
One of the biases of the research was the uncertainty of the truthfulness of the answers, since the study did not follow the course of treatment. What was answered by the participants cannot translate what was truly accomplished.
Another limitation is that most of them have low income and low education, which may influence the quality of responses for lack of a true understanding of the process.
It is necessary to encourage the development of new studies related to the theme, with other methodologies to explore more thoroughly the factors that determine adherence to self-care, contributing to the elucidation of these gaps.
BIBLIOGRAPHY
1.Instituto Nacional de Câncer José Alencar Gomes da Silva (Br). Estimativa 2014: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2013.
2.Pires AMT, Segreto RA, Segreto HRC. Avaliação das reações agudas da pele e seus fatores de risco em pacientes com câncer de mama submetidas à radioterapia. Rev Latino-Am Enfermagem 2008; 16: 844-9.
3.Frigato S, Hoga LAK. Assistência à mulher com câncer de colo uterino: o papel da enfermagem. Revista Brasileira de Cancerologia 2003; 4(49): 209-14.
4.Araújo CRG, Rosas AMMTF. A consulta de enfermagem para clientes e seus cuidadores no setor de radioterapia de hospital universitário. Revi enferm UERJ. 2008; 16: 364-9. [citado em 29 abr. 2014] Disponível em: http://www.facenf.uerj.br/v16n3/v16n3a11.pdf.
5.Guedes MTS, Blecha FP. Tratamento de radiodermatite no cliente oncológico: subsídios para intervenções de enfermagem. Revista Brasileira de Cancerologia. 2006; 2(52): 151-63.
6.Instituto Nacional de Câncer José Alencar Gomes da Silva (Br). Ações de enfermagem para o controle do câncer: uma proposta de integração ensino-serviço. 3ª ed. Rio de Janeiro: INCA; 2008.
7.Araújo CRG, Rosas AMMTF. O papel da equipe de enfermagem no setor de radioterapia: uma contribuição para a equipe multidisciplinar. Revista Brasileira de Cancerologia. 2008; 3(54): 231-7.
8.Naylor W, Mallet J. Management of acute radiotherapy induced skin reactions: a literature review. Eur J of Oncol Nurs. 2001; 4: 221-3.
9.Conselho Federal de Enfermagem (Br). Resolução nº 159/1993. Dispõe sobre a consulta de enfermagem. Rio de Janeiro: COFEN; 1993.
10.Conselho Federal de Enfermagem (Br). Resolução nº 211/1998. Dispõe sobre a atuação dos profissionais de enfermagem que trabalham com radiação ionizante. Rio de Janeiro: COFEN; 1998.
11.Marconi MA, Lakatos EM. Fundamentos de metodologia científica. 7ªed. São Paulo: Atlas; 2010.
12.Gil AC. Como elaborar projetos de pesquisa. 5ª ed. São Paulo: Atlas; 2010.
13.Ministério da Saúde (Br). Conselho Nacional de Saúde. Resolução nº466/12: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF): Conselho Nacional de Saúde; 2012.
14.Instituto Nacional de Câncer José Alencar Gomes da Silva (Br).[site de internet]. Fatores de risco para o câncer. [citado em 29 abr 2014] Disponível em: http://www1.inca.gov.br/conteudo_view.asp?id=322.
15.Alvarenga LM, Ruiz MT, Bertelli ECP, Ruback MJC, Maniglia JV, Bertollo EMG. Avaliação epidemiológica de pacientes com câncer de cabeça e pescoço em um hospital universitário do noroeste do estado de São Paulo. Rev Bras Otorrinolaringol. 2008; 74: 68-73.
16.Trindade BM, Campos RTP. Sistema computacional para dosimetria de nêutrons e fótons baseado em métodos estocásticos aplicado a radioterapia e radiologia. Radiol Bras. 2011; 44: 109-16.
17.Ferreira NML, Souza MBB, Costa DB, Silva AC. Integridade cutâneo-mucosa: implicações para a família no cuidado domiciliário ao doente com câncer. Rev enferm UERJ. 2009; 17: 246-51.
18.Smeltzer, SC, Bare, BG. Tratado de enfermagem médico-cirúrgica. 11ª ed. Rio de Janeiro: Guanabara Koogan; 2009.
19.Cuppari L. Nutrição clínica no adulto. 2ª ed. São Paulo: Manole; 2005.
20.Dealey C. Cuidando de feridas: um guia para as enfermeiras. 3ª ed. São Paulo: Editora Atheneu; 2008.
21.Reis PED, Carvalho EC, Bueno PCP, Bastos JK. Aplicação clínica da Chamomilla recutita em flebites: estudo de curva. [citado em 29 abr 2014] Rev Latino-Am Enfermagem. 2011;19:[08 telas] Disponível em http://www.redalyc.org/articulo.oa?id=281421953002.
22.Piper BF, Dibble SL, Dodd MJ, Weiss MC, Slaughter RE, Paul SM. The revised Piper fatigue scale: psychometric evaluation in women with breast cancer. Oncology Nursing Forum. 1998; 25 677-84.
23.Leite FMC, Ferreira FM, Cruz MAS, Lima EFA, Primo CC. Diagnósticos de enfermagem relacionados aos efeitos adversos da radioterapia. Rev Min Enferm. 2013; 17: 940-5.
24.Luna NSA, Baeza MR, Castell EC, Santos FC, David HL, Castillo MMA. Intervención educativa: implementación de la agencia de autocuidado y adherencia terapéutica desde la perspectiva del paciente diabético. Rev enferm UERJ. 2013; 21: 289-94.
25.Machado MMT, Leitão GCM, Holanda FUX. O conceito de ação comunicativa: uma contribuição para a consulta de enfermagem. Rev Latino-Am Enfermagem. 2005; [citado em: 29 abr 2014]13: 723-8. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692005000500017&lang=pt.
26.Cavalari E, Nogueira MS, Coelho SMLF, Cesarino CB, Martin JFV. Adesão ao tratamento: estudo entre portadores de hipertensão arterial em seguimento ambulatorial. Rev enferm UERJ. 2012; 20: 67-72.