(*) p-value for the Chi-square Test
RESEARCH ARTICLES
Falls in older adults living at home and their association with daily living activities
Rosalina Aparecida Partezani RodriguesI; Suzele Cristina Coelho Fabricio-WehbeII; Marina Aleixo DinizIII; Jack Roberto Silva FhonIV; Aline Francesco da SilvaV
I
Professor in the Department of General and Specialized Nursing at the Ribeirão Preto College of Nursing of the University of São Paulo. Ribeirão Preto, São
Paulo, Brazil. Email: rosalina@eerp.usp.br
II
Postdoctoral research fellow in the Department of General and Specialized Nursing at the Ribeirão Preto College of Nursing of the University of São Paulo.
Ribeirão Preto, São Paulo, Brazil. Email: suzelecris@ig.com.br
III
PhD student in the Department of General and Specialized Nursing at the Ribeirão Preto College of Nursing of the University of São Paulo. Brazil. Email: marinadiniz@usp.br
IV
PhD student in the Department of General and Specialized Nursing at the Ribeirão Preto College of Nursing of the University of São Paulo. Ribeirão Preto,
São Paulo, Brazil. Email: beto_fhon@hotmail.com
V
Graduate student in the Collaborating Centre of the World Health Organization for Development of Nursing Research, at the Ribeirão Preto College of Nursing
of the University of São Paulo. Ribeirão Preto, São Paulo, Brazil. Email: alinefrancesco@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.10406
ABSTRACT
This cross-sectional study, to determine the prevalence of falls in older adults living at home, and to identify the level of dependence in activities of daily living among those who fell and those who did not, was conducted using a two-stage cluster sample of 230 individuals of both sexes, aged over 70 years, in Ribeirão Preto, São Paulo, in 2013. Social profile, falls, Lawton & Brody scale and Katz Index were investigated. Falls were identified in 37.8% (1-7, sd=1.0) of individuals interviewed. Falls were more prevalent among women (25.2%), and younger individuals (23%). No association was found between falls and Instrumental Activities of Daily Living, although there was an association between falls and Activities of Daily Living, as those who fell were more dependent on these activities. The study of these activities is suggested as a strategy to prevent falls.
Keywords: Older adults; accidental falls; activities of daily living; geriatric nursing.
INTRODUCTION
The world population is rapidly aging. Between 2000 and 2025, the proportion of older people over 60 years old will increase from 700 million to 1200 million1.
Therefore, knowledge about the aging process and recognition of health care for the elderly with the aim to guarantee autonomy and independence, and prevent multiple adverse events, are important tools for the provision of comprehensive care of this population2.
Falls, which are common adverse events among older people, are an important public health problem due to their high frequency and serious consequences that can result in high social and economic costs2. Falls can be associated with decreased functional capacity of an elderly individual, and lead to decreased quality of life.
The aim of the present study was to determine the prevalence of falls among older people living at home, and compare the level of dependence for activities of daily living (ADL) between older people who fell and those who did not.
Provided with this information, the researchers believe that it would be possible to verify whether ADL can be used as a tool in a broad geriatric assessment to prevent falls among the elderly. It is important to investigate the functional capacity of elderly individuals through analysis of their capacity to carry out these activities. This study is expected to support public health care policies for older people, with regard to the importance of preventing falls through promotion of functional capacity of this population, to ensure autonomy and independence in performing ADL. The authors hope this study can contribute to disseminate data and understanding of the elderly, and encourage special attention to their health and self-care.
LITERATURE REVIEW
Fall can be defined as an involuntary event in which an individual loses their balance and falls to the floor or another hard surface. They can cause mild or serious injury and even death3.
Each year, more than one-third of elderly individuals aged 65 years or older who live in the community suffers a fall. Among elderly people aged 70 years, this ratio is 32-42%, and for those 80 years or older this value is 50%, indicating that falls become more common with the advance of age 4. Furthermore, one-third of the elderly population suffers one or more falls per year, being three times more frequent in women compared to men. However, overall mortality associated with this condition is greater in males5.
Worldwide, falls currently represent 12% of deaths among the elderly, and 40% of deaths from injury in this age group. They are the fifth leading cause of death in old age, and the first from external cause5-7. Approximately 5% to 10% of all falls among older people living in the community result in fracture and serious injury to soft tissue and/or the head, and more than 30% of elderly individuals that fall experience a decline in their functionality8-10.
Falls can have various types of consequences for an elderly person, such as: physical, that impede activities of daily living and increase risk of death; psychological, that may be related to the fear of falling syndrome; economic and social, that generate costs for the elderly and society, and hinder interaction with other people outside of the home environment11-15.
In clinical practice, it is verified that declines in functional capacity of elderly individuals can both lead to fall and be caused by this event. Functional capacity can be defined as the physical and mental skills necessary for an individual to maintain an independent and autonomous life, i.e. they have no need for assistance with basic activities of daily living (BADL) and instrumental activities of daily living (IADL)16,17. Therefore, evaluation of these indicators should be considered when planning health care actions to prevent falls. Maintenance of autonomy and independence of the elderly in performing ADL is essential to ensure their quality of life.
METHODOLOGY
This was an observational and cross-sectional study, whose sample was selected in the project Health and living conditions of older people from Ribeirão Preto, São Paulo, undertaken in 2008, in the urban area of the city of Ribeirão Preto, in the Brazilian state of São Paulo, with older people aged 65 years or older, who lived in the community.
The cluster and two-stage sampling procedure was probabilistic. In the first stage, the census sector was the primary sampling unit (PSU) considered. Thirty census sectors were randomly selected, with probability proportional to the size of number of households, among the 600 census sectors of the municipality. The second stage was to visit a fixed number of households in order to ensure the sampling self-weighting, with randomized selection of the street and block where this search process was initiated. To attain the number of elderly people in the sample, at least 110 households were visited in each sector.
After random selection of the sectors and identification of the districts, the streets of each sector selected were listed and another drawing was performed to determine which streets would be visited by the interviewers. All of the elderly individuals were removed from the sample after three visits by the interviewer. The interviews were conducted in clockwise order, on the blocks selected from the sectors.
After 110 households had been interviewed in each sector, if the intra-household density had not been attained, the interviewers continued the visits until they attained the desired number of older adults participants by sector.
Before performing the search for households, the researchers traveled the sectors selected to update the number of households, by sector, in 2007, since the information used was related to the 2000 census. After the search, there were no significant changes to the number of households.
In 2008, 515 older adults were interviewed. In the first half of 2013, these individuals were contacted by telephone to schedule a visit for interview. Two hundred and thirty older adults participated in the study. Deaths totaled 101 (19.6%) and losses due to change of address, refusal to participate, institutionalization and absence of the individuals at home (after three visits) totaled 184 (35.7%).
Data were collected in the homes of the elderly individuals by trained interviewers (undergraduate and graduate students), in uniform and duly identified by badges. Personal information and social profile were collected by means of an instrument developed by the Research Group in Geriatric and Gerontological Nursing of the Ribeirão Preto College of Nursing at the University of Sao Paulo (NUPEGG). Cognition was evaluated through application of the Mini-Mental State Exam (MMSE), translated and adapted to Brazilian Portuguese18, with scores ranging from 0 to 30 points. For data analysis, this variable was dichotomized in without and with cognitive deficit, using the cutoff point suggested by the authors of the instrument referenced above, being 13 for those identified as illiterate; 18 for those with low/average level of education; and 26 for highly-educated individuals.
The investigation of falls was performed using an instrument19 that investigates the context, causes and consequences that a fall may cause to an elderly individual.
The Katz Index adapted to Brazilian Portuguese20 was used for evaluation of BADL. This index consists of six items that measure the performance of an individual in self-care activities, which follow a hierarchy of complexity as follows: eating, sphincter control, transfer, personal hygiene, and ability to dress and bathe. For investigation of the IADLs, Lawton and Brody's scale, adapted to the Brazilian context, was used21.
The collected data were entered into the Microsoft Excel® software. After coding of all variables in a dictionary, a database was developed that was fed using the technique of double-entry validation. After their entry and validation for consistency, the data were imported into the software application Statistical Package for the Social Sciences for Windows, v19.0.
All variables underwent statistical analysis. For qualitative or categorical variables, simple frequency measurements were used, and for quantitative variables, analyses with measurements of central tendency (mean and median) and dispersion (standard deviation) were used. An association test (Chi-square) was performed, and logistic regression was used to quantify the association.
The study was carried out in compliance with Resolution CNS 466/12 of the National Commission of Ethics and Research of the Brazilian Ministry of Health, and was approved by the Research Ethics Committee of the Ribeirão Preto College of Nursing in Opinion No. 01852512.6.0000.5393. A free and informed consent form was prepared adhering to Resolution CNS 466/12, and before the start of each interview, it was read and signed by the participants and/or their caretaker/family member in two copies (one for the researcher, and the other for the participant).
RESULTS AND DISCUSSION
Of the 515 older people visited, 230 (44.6%) agreed to participate in the study and were interviewed. Of these, 65.7% were female and 42.6% were widowed. The participants' mean age was 79 years (70-103 years; SD=6.23), and the majority had a mean level of education of 1 to 4 years (55.8%), and individual monthly income from between R$501.00 to R$1,000.00 (53.9%) (See Table 1 below).
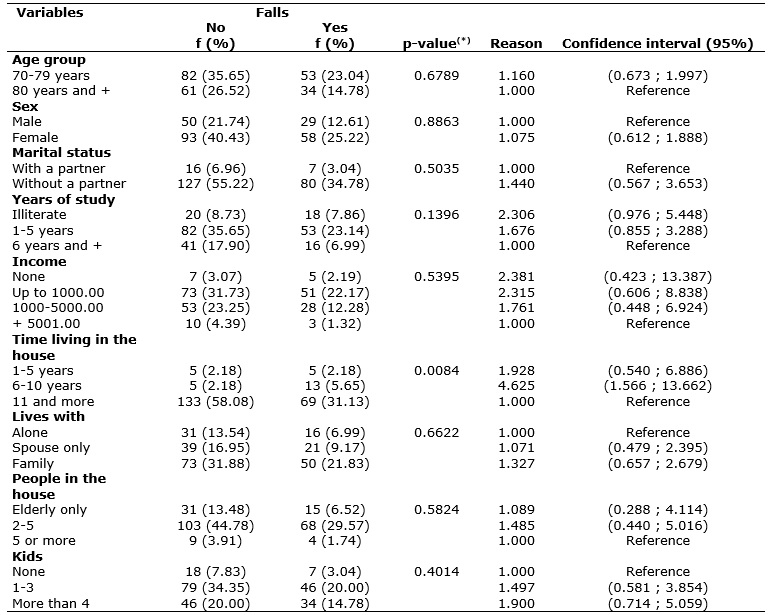
TABLE 1:
Test of association and logistic regression between falls and socio-demographic variables of older adults living at home. Ribeirão Preto, São Paulo,
Brazil, 2013. (N=230)
(*)
p-value for the Chi-square Test
Among the respondents, 37.8% had suffered at least one fall (1-7 falls; SD=1.0). Falls were more prevalent in females (25.2%), in younger-older adults (23%), subjects living without a partner (34.7%), with 6 to 10 years of study (23.1%), with an individual income of up to R$ 1,000.00 (21.93%), who lived with relatives (21.8%), and had between 1 and 3 children (20%), as shown in Table 1.
The prevalence of falls found in the present study, and the greater occurrence of falls in women, are consistent with data in the literature4,5. In another cross-sectional study carried out with 240 older adults living at home in the city of Ribeirão Preto, the prevalence of falls was 33.3%, with higher incidence in women22. Other national studies on the subject found a similar prevalence between 31.2% and 59.3%2,23, and this percentage was around 19.1 % to 31.78% in international studies24,25.
The data obtained in the present study also showed that falls were more prevalent among younger-older adults (60-79 years), which corroborates another national study22, but differs from other studies4,26 that found that falls were more prevalent in older-older adults (80 years and older). This difference may be attributed to the fact that younger-older adults are more active in activities for daily living, and therefore are more susceptible to fall-related risk factors. It can be assumed that older-older adults are more guarded and less exposed to dangers in their daily activities. Older-older adults may also be more guarded with regard to trigger factors of falls, such as environment and clothing.
No association was verified between fall and most of the socio-demographic data investigated. In this regard, the only association found was between falls and time living in the same house (p 0.0084). It was verified that older adults who had lived in the same house from 6 to 10 years were 4.6 times (CI-1.566; 13.662) more likely to fall when compared to those who had lived in the same house for 11 years and longer. It is important to note that although no association was found between falls and years of study, it was found that the chance of a fall decreased as years of study increased. Illiterate older adults were 2.3 (CI 0.976; 5.448) times more likely to fall than those with 6 years or more of education. The same occurred when the association between falls and income was analyzed, which was not verified; however, it was observed that older adults with no income were 2.38 times (CI 0.423; 13.387) more likely to fall than those with income over R$ 5,000.00 R$, verifying that the higher their income, the lesser their chance of falling.
Among the elderly who suffered falls, 76.4% fell from a standing position, this being the most prevalent kind of fall for both males (65.5%) and females (81.03%). As for location of the fall within the home, the backyard (20.0%) had the highest occurrence, and outside the home, the street had the highest occurrence (16.25%).
In a study carried out in Rio de Janeiro, most of the falls recorded occurred at home27. In Belo Horizonte, among the elderly who suffered a fall, 48.44% fell from a standing position, and the location of greatest occurrence of falls was the backyard (12.5%)23. In Spain, a study with 363 older adults found that 73.4% of falls occurred in a place known by the individual and, among these, 55.3% occurred at home25.
The most prevalent intrinsic factors cited as responsible for the falls were: shifting balance (29.9%); difficulty walking (12.6%), muscle weakness (11.6%) and dizziness (6.9%). Among the most cited extrinsic factors were: inadequate footwear (39.1%); slippery floors (17.2%); irregular floors (10.3%); high steps (5.7%) and objects on the floor (5.7%).
A fall is a multifactorial event that entails biological, behavioral, social and environmental factors, and involves intrinsic and extrinsic aspects 28-30. Evidence in the literature points to the existence of approximately 400 different risk factors for falls. At least two concurrent health conditions and one environmental factor played a decisive role in most cases of falls among the elderly5. The prevalence of falls among older adults living at home and that have at least one risk factor for fall was 27%, and increased to 78% among those with four or more associated factors 31,32. Thus, behind each fall was the association between the multiple systems and organs dysfunction and the influence of aspects external to the individual33.
Falls related to extrinsic factors emphasize the possibility of educational actions to be implemented in a preventive approach. It is necessary to modify domestic environments to minimize the dangers, as well as to promote health, prevent disease and disability in the elderly, with the goal of reducing the risks that may propitiate falls22.
It was noted that among the older adults who had fallen in the present study, the main consequence cited was being afraid of falling again, followed by affected walking, hospitalization and needing help with activities. These consequences are consistent with the results of other studies. Worldwide, falls account for 87% of fractures and 50% of hospitalizations among the elderly3. In the United States, 25.6% of a sample of 5,681 older adults had fallen, and among these, 61% showed some kind of injury and 20% were hospitalized34. In Brazil, a study with 2,209 older adults (aged ≥60 years) living at home identified a prevalence of falls of 27.1%, and 8.7% for recurrent falls35. Another study of 6,616 elderly Brazilians aged 65 years and older verified a frequency of falls of 27.6%, 11% of which resulted in fracture and 1% in surgical care 36.
The literature indicates that elderly people generally have a low sense of effectiveness to avoid falling, are afraid of falling, are restricted in their activities and experience loss of self-confidence37. Post-fall syndrome and fear of falling affect 73% of those who fell in the previous year, and among the elderly with no reports of recent falls, the prevalence was 46%38. Thus, fear of falling can result in a post-fall syndrome including dependence, loss of autonomy, immobilization, isolation and depression, which will lead to greater restrictions in ADL 39.
Independence, understood as the ability to perform BADLs and IADLs autonomously, with little or no help from others, involves functional capacity. Independence allows the individual to take action regarding decisions about how to live daily, according to their own preferences and rules16.
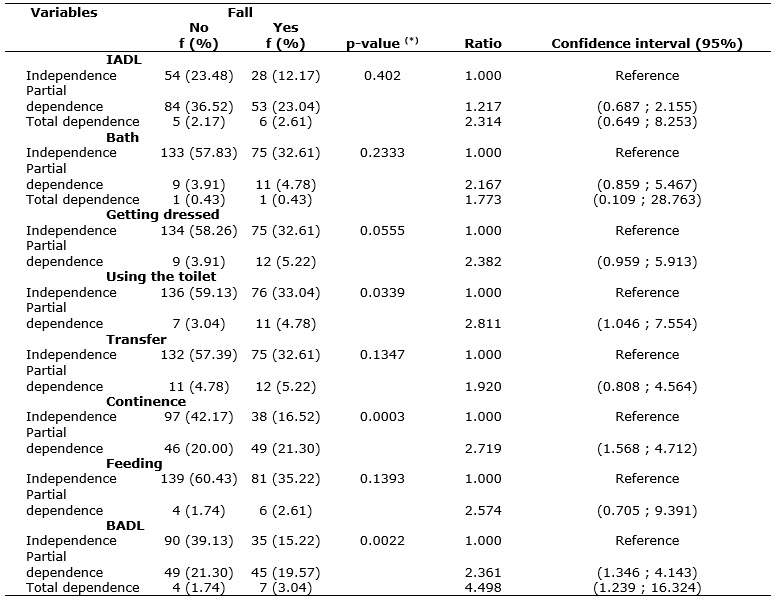
In the present study, no association was verified between a fall and IADLs, as seen in Table 2. However, there was evidence that independent older adults (23.48%) were more prevalent among those who did not fall, and total dependence (2.61%) was more prevalent among those who suffered a fall. It was also found that older adults with total dependence were 2.314 (0.649; 8.253) times more likely to fall, when compared to older adults with independence.
TABLE 2:
Test of association and odds ratio between falls, IADL and BADL in older adults living at home. Ribeirão Preto, São, Brazil, 2013. (N = 230)
(*)
p-value for the Chi-square Test
With regard to BADLs, the same association was verified with falls. Additionally, participants with total dependence had a chance of falling of 4.498 (CI 1.239; 16.324) compared to those who were independent for these activities, i.e., the higher the dependence for these activities, the greater the risk of falling. Among the activities investigated in the evaluation the BADL, those most associated with fall were continence and using the toilet.
It is possible to infer that this finding may be related to the fact that IADL are more complex and elaborate, and require more cognitive skills than motor. Thus, IADL can be activities less performed by older adults compared to BADL.
The multidimensional assessment of older people makes it possible to identify disabilities and limitations as care needs, targeting interventions 40. This type of evaluation emphasizes the functionality of an older adult. In this evaluation, it is necessary to include the health history of the individual, assessment of physical function, sensory (hearing and vision) component analysis, measurements of orthostatic and neurological signs, musculoskeletal assessment, cognitive dysfunction and depression14.
Assessment of ADL can assist in this multidimensional investigation of the elderly, because BADL can be a strong indicator that the elderly needs greater attention and care to prevent falls. It is inferred that promoting and recovering autonomy and independence of older people in their execution of these activities can be a strategy to prevent falls. However, this statement needs to be further investigated in cohort studies that quantify how this strategy can be effective for prevention.
CONCLUSION
The data from the present study reinforce the importance of knowing the context of a fall, identifying factors involved in this event and the consequences that it may entail, to outline preventive strategies in the face of this event that is so common among the elderly.
The main limitation of this study was its cross-sectional design, which makes the ordering of causality among the variables impossible. However the response percentage and the fact that the sample is derived from a population-based study increases the relevance of the study.
Based on the evidence of this research, it is suggested that the investigation of BADL be used as a strategy to prevent falls. Once the deficiency is identified in the implementation of these activities, it is necessary to use interventions to recover and promote the independence of older people to promote autonomy and independence.
Falls among the elderly are a complex and multifactorial event, the prevention of which is necessary and constitutes a challenge to older adults themselves, families, healthcare professionals and public policies.
REFERENCES
1. Organización de Las Naciones Unidas. Report of her second world asemblea el envejecimiento. Madrid (Es): Naciones Unidas; 2002.
2. Cross DT, LK, MT, Teixeira MTB, Bastos RR., ICCG Milk. Prevalence of falls and associated factors in elderly individuals. Rev Saude Publica. 2012; 46:38-46.
3.World Heath Organization (WHO). World Heath Organization Report: prevention of falls in older age. Geneva (Swi): Who; 2007.
4. PM Ciaschini, Straus, Dolovich LR, Goeree RA, Leung KM, Woods CR et al. Community-based intervention to optimise falls risk management: a randomised controlled trial. Age and Ageing. 2009; 38:724-30.
5. Czerwinski and Białoszewski D, Borowy p., Kumorek, Białoszewski a. Epidemiology, clinical significance, costs and fall prevention in elderly people. Ortop Traumatol Rehabil. 2008; 10:419-28.
6. Kwan MM, Close JCT, Wong AKW, Lord MR. Falls incidence, risk factors, and consequences in chinese older people: a systematic review. JAGS. 2011; 59:536-43.
7. Goins RT, Innes K, Dong l. Lower body functioning prevalence and correlates in older american indians in the southeastern tribe: the native elder care studs. J Am Geriatr Soc. 2012; 60:577-82.
8. Wang J, Chen Z, Song Y. Falls in aged people of the Chinese mainland: epidemiology, risk factors and clinical strategies. Ageing Res Reviews. 2010; 13-7.
9.Bleijlevens MHC, Diederiks JPM, Hendriks MRC, van Haastregt JCM, Crebolder HFJM, van Eijk jthm. Relationship between location and activity in injurious falls: an exploratory study. BMC Geriatrics. 2010; 10:40.
10. Langlois F, Vu TTM, Kergoat M, Chassé K, Dupuis G Bherer, l. The multiple dimensions of frailty: physical capacity, cognition, and quality of life. Int Psychogeriatrics. 2012; 24:1429-36.
11. Zijlstra GAR, van Haastregt JCM, van Eijk JTM, van Rossum E, Stalenhoef PA, Kempen GIJM. Prevalence and correlates of fear of falling, and associated avoidance of activity in the general population of community-living older people. Age and Ageing. 2007; 36:304-9.
12. Rajan AP, Sharif ER, Atie S, Souza AC, Schilithz to. The influence of the falls on the quality of life of older adults. Ciênc public health. 2008; 13:1264-73.
13. Freiberger and Vreede p. Falls recall: limitations of the most used inclusion criteria. Eur Rev Aging Phys. Act. 2011; 8:105-8.
14.Al-Aama t. Falls in the elderly: spectrum and prevention. Can Fam Physician 2011; 57: 771-6.
15. Before DL, Schneider IJC, Benedetti TRB, orsi e. Fear of falling and associated factors in recurrent old of Florianopolis, Santa Catarina, Brazil. Cad Saúde Pública. 2013; 29:758-68.
16. Scott MJ, Lee MVO, Ahmad MFM, Morales GLA. Assessment of the degree of dependence in activities of daily living in elderly of the city of Fortaleza-Ceará. Acta Paul Enferm. 2006; 19:201-6.
17.Fiedler MM, Peres KG. Functional capacity and associated factors in elderly people in southern Brazil: a population-based study. Cad Saúde Pública. 2008; 24:409-15
18. Bertolucci PHF, SMD, Brucki Campacci Sir, JulianoY. The mini mental state examination in a general population. Impact of schooling. ARQ Neuropsiquiatr. 1994; 52:1-7.
19. Schiaveto FV. Assessment of the risk of falls in the elderly in the community [dissertation]. Ribeirão Preto (SP): University of São Paulo; 2008.
20. Lino VTS, Pereira SRM, Camacho LAB, Raja FST, Buksman n. cross-cultural adaptation of the scale of Independence in activities of daily living (Katz). Cad Saúde Pública. 2008; 24:103-12.
21. Santos RL, Virtuoso Jr JS. Reliability of the Brazilian version of the instrumental activities of daily living. RBPS. 2008; 21:290-6.
22. Fhon JRS, Fabrício-Wehbe SCC, TRP, Stackfleth R Vendruscolo's experience, Mahmoud S, Rao RAP. Accidental falls in the elderly and their relation with functional capacity. Rev Latino-Am Nursing. 2012; 20:927-34.
23. Chianca TCM, Andrade CR, Albuquerque J, Wenceslau LCC, Thaddeus LFR, Macieira TGR. et al. Prevalence of fall in older adults enrolled in the health center of Belo Horizonte – MG. Rev Bras Enferm. 2013; 66:234-40.
24. The Skalska, Wizner B, K Piotrowicz, Klich-Raczka, Klimek and Mossakowska m. et al. The prevalence of falls and their relation to visual and hearing impairments among the nation-wide cohort of older poles. Experimental Gerontology. 2013; 48:140-6.
25. Sticks-Fabra F, Castro, ME Pérula TLA, Fernández FMJ, Moral RR, Enciso BI. Saggy in elder de la comunidad: prevalence, consequences y asociados factors. Primary Attention. 2006; 38:450-5.
26. Nicolussi BC Fhon JRS, Santos CAV, Kusumota L, Marques S, Rao RAP. Quality of life in elderly people that have suffered falls: integrative literature review. Ciênc public health. 2012; 17:723-30.
27. Chris ESF, Bloch KV, Rodrigues LC. Characteristics and general circumstances of falls leading to severe fractures in elderly people in Rio de Janeiro, Brazil. Cad Saúde Pública. 2009; 25: 455-9.
28. Abdullah ST, Soldera CLC, Carli GA, Garcia I, Raj l. analysis of extrinsic and intrinsic factors that predispose to falls in the elderly. Rev Assoc Med Bras. 2012; 58:427-33.
29. Fox PJ, Vazquez L, Tonner C, Stevens JA, Fineman N, Ross LK. A randomized trial of the it is multifaceted intervention to reduce falls among community-dwelling adults. Health Education Behavior. 2010; 37:831-48.
30. Stevens JA, Baldwin GT, Ballesteros MF, Noonan RK, Sleet. An older adult falls research agenda from the public health perspective. Clin Geriatr Med. 2010; 26:767-79.
31. American Geriatrics Society and the British Geriatrics Society (AGS and BGS). Summary of the updated American Geriatrics Society/British Geriatrics Society. Clinical practice guideline for prevention of falls in older persons. New York: AGS/BGS; 2010.
32. Tinetti ME, Kumar C. The patient who falls: "it's always a trade-off." JAMA. 2010; 303:258-66.
33. Gschwinda YJ, Wolfa I, Bridenbaugha SA, Kressig RW. Basis for the Swiss perspective on fall prevention in vulnerable older people. Swiss Med Wkly. 2011; 141: w13305, 2011.
34. Milat JA, Watson WL, C Monger, Barr M, Termeer M, Reid, m. Prevalence, general circumstances and consequences of falls among community-dwelling older people: results of the 2009 NSW Falls Prevention Baseline Survey. NSW Public Health Bulletin. 2011; 22:43 -8.
35. Chen AMV, Ricci, Coimbra IB, Costallat LTL. Falls in the elderly of the family health program. Arch Gerontol Geriatr. 2010; 51:317-22.
36. Seng FV, Facchini LA, DS Senanayake, Piccini RX, Tomasi and Thumé, e. et al. Prevalence of falls in the elderly in Brazil: a national analysis. Cad Saúde Pública. 2011; 27:1819-26.
37.Scheffer AC, Schuurmans MJ, Dijk NV, Hooft TV, Rooij . Fear of falling: measurement strategy, prevalence, risk factors and consequences among older persons. Age and Ageing. 2008; 37:19-24.
38. Fabre JM, Ellis R, Kosma M, Wood R.H. Falls risk factors and a compendium of falls risk screening instruments. J Geriatr Phys Ther. 2010; 33:184-97.
39.Organização Mundial Da Saúde. The who global report on the prevention of falls in old age. São Paulo: Secretary of State for Health Sao Paulo; 2010.
40. AGS Coast, Costa FBC, Oliveira ARS, Silva VM, Ahmad TL. Occurrence of falls and body mass index in the elderly. Rev Nurse UERJ. 2013; 21:508-14.