REVIEW ARTICLES
Concept analysis of behavior prevention in the context of chronic disease
ABSTRACT: Concept analysis proves important to improving the understanding of a given phenomenon and to supporting professional practice. This study aimed at analyzing the concept of prevention behavior in the context of chronic disease on the basis of the model referred by Walker and Avant in 2005. In 2011 an integrative review on databases was performed with combinations of descriptors. Online articles addressing the questions made were selected. Thereby, 146 abstracts were read and 25 publications were selected. Elements of the phenomenon were identified as attributes: skill, knowledge, and attitude; antecedents: disease occurrence, identification of risk factors, decision making, and support network; and consequences: individual self-management, mastery of skills, adaptation, and improvement in quality of life. As a result, it was possible to formulate a wider concept of behavior prevention, which, on its turn, can help the health professional in preventive action.
Keywords: Concept formation; behavior; prevention & control; stroke
INTRODUCTION
Sometimes, countless individuals have mistaken understanding with regard to certain common concepts in a professional environment, for example. In this way, research studies and analysis of the concept of specific elements are important, in order to clear and comprehensive understanding of literature.
In this context, we highlight the prevention behavior phenomenon, given the need for modifications to lifestyle of people who experience chronic disease like stroke. Prevention behavior is important for dealing with phenomena of promoting a healthy lifestyle, in order to avoid complications and aggravations, reduce costs and demand at health services1,2.
So, with the goal of improving the health condition or prevent occurrence of worsening, behavior of prevention focuses on, in general, the management of risk factors3.
Although some of these risk factors are physiological nature, in which stands out the pharmacological action, the risk factors that can be controlled through the modification of habits of the individual call the attention. Mainly knowing that habits are aspects quite susceptible to variation, according to cultural issues, beliefs and values, it should be considered in definition4.
Based on the importance of conceptual understanding of the phenomenon, it is considered the chosen technique concept analysis to assist the use of thought and communication, as well as describe particular strategies, especially when the concept is vague or has more than one meaning5.
It is necessary concept analysis for the case of careful examination and a descriptive word or phrase and its use in the language, along with explanation of how it is and how it relates to other words or terms in the transmission of actual and possible meanings6.
Thus, the objective of this study was to analyze the concept of preventive Behavior in the context of chronic disease and based on the model advocated for conceptual analysis6, which was chosen because it is more directed to the nursing classification systems. It is intended, therefore, to seek a more meaningful and consistent understanding possible about the concept, contributing to better understanding of professionals, among which stands out the figure of the nurse health promoter, directly responsible for the ongoing management of modifiable risk factors of chronic patients.
METHODOLOGY
This study is of Integrative Review type, which sought to evaluate the existing literature thoroughly for providing subsidies to the analysis of concept proposal. The study was conducted during the period of September to November 2011.
Given the analysis of concept provide the identification of particular and characteristic attributes of the concept, it is important to use procedures described by a consolidated model as what was used in the study in question6. It should be noted that the analysis of concept, according to the authors6, refers to the modified and simplified proposal from another more general model and previously proposed5.
So, eight recommended steps were followed as sufficient to capture phases and implementation of the essence of the process from concept analysis to reality of nursing taxonomies, comprising: selecting a concept; determination of the goals or purposes of analysis; identification of uses of concept; determination of the attributes that define it; identification of a case model; identification of a limit case, a related case, otherwise, an event invented and a legitimate case; identifying antecedents and consequent; and definition of empirical references6. It should be noted that this study did not take place to identify the cases suggested by the authors, following the other steps, that were enough for the preparation of the concept in question.
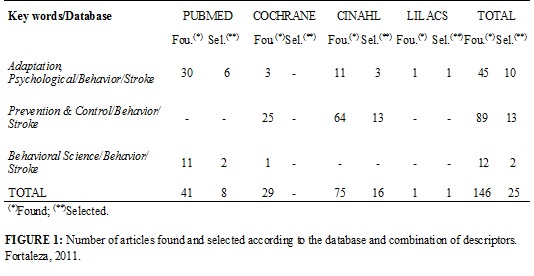
Thus, for search of evidence about this concept in the literature, an integrative review of literature in databases was done: Publications Medical (PUBMED), Cummulative Index to Nursing and Allied Health Literature (CINAHL), Latin American literature and Caribbean Health Sciences (LILACS)and Cochrane library (CLIB), with three combinations of indexed descriptors: Behavior, Adaptation, psychological and Stroke; Behavior, Prevention & control and Stroke; and lastly Behavior, Behavioral Science and Stroke.
It is mentioned that cerebral vascular accident or stroke is focused because it is a chronic disease that requires significant modifications of individual habits, given the range of physical sequels and limitations imposed by stroke.
In this search were found 146 articles, which were submitted to a reading of the title, as well as the abstract, in order to verify whether they would respond to any of the following questions: what is understood by prevention behavior of the patient or family member after the stroke event? Which elements are characterized as prevention behavior? What factors hinder or affect the behavior?
In addition to the need of the possibility of at least one of the questions referred, it is established the following inclusion criteria: to be published in Portuguese, English or Spanish language and be available in their entirety and electronically. Articles may be repeated were deleted.
Thus, a total of 25 articles was selected, of which 16 were found on base CINAHL1-3,7-19, eight articles were selected from the PUBMED4,20-26 basis and a LILACS27 database, as shown in Figure 1.
It is highlighted that many publications, especially those of the Cochrane database, referred to behavioral aspects of prevention with emphasis on pharmacological mechanisms. Thus, these studies were excluded because they did not meet the objectives of the research.
RESULTS AND DISCUSSION
We analyzed 25 publications that subsidized the identifying attributes, antecedents and consequences as well as definitions about the concept of Preventive Behavior.
Thus, the integrative review conducted, it was possible to identify various aspects of the concept of preventive behavior, compile the data and build a final broader concept than those found, since no studies presented complete concept and often this is implicit and dissolved in the text. Thus, among the 25 works analyzed, 16 had direct information about the definition of the concept, the other articles1,3,8,12,13,18,19,22,25 were the other important aspects to the elaboration of the concept as attributes, antecedents or consequences.
As noted, many definitions are similar in some aspects and complement each other, so that the concept of prevention behavior impounded refers to subjective and intrinsic aspects of the individual. Such aspects are based on the correct identification of risk factors or health modifiable conditions15, by developing skills and individual competencies14,15 to provide effective management fators14,27. See Figure 2.
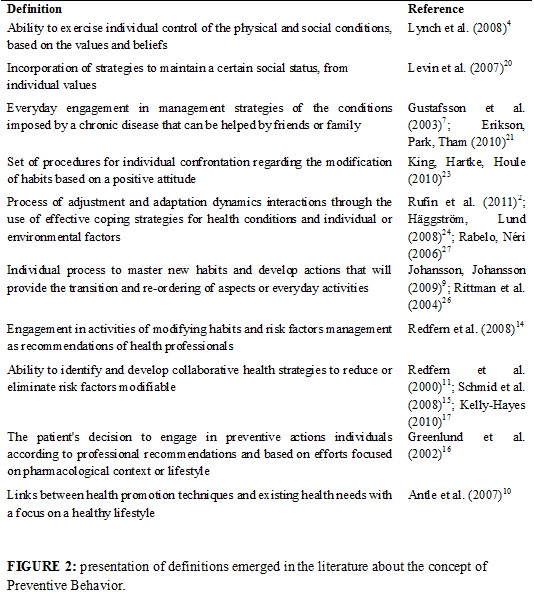
It should be noted that the behavior of prevention is understood as a continuous process of transition and reorganization of activities and routine aspects of the person26. Routine aspects can be perceived as an individual's habits, thus, modification or acquisition of new habits also occurs in some definitions found9,14.
As the definitions found, it was perceived congruence studies to refer to the behavior of prevention, in face of the acquisition or modification of everyday habits, through the acquisition of skill. It should be noted that the development of ability relates to the process of knowledge acquisition that is configured as dynamic and continuous. Such a process is also likely to use health promotion strategies for the effective confrontation of health situations10,27. Knowledge is thus related to the development of skills for more effective management of the risk factors experienced by the individual3,7.
Health situations are translated by risk factors, with focus on that are modifiable and, are related to individual conditions, such as the person's habits. There are also environmental conditions, which in the context of the occurrence of falls, it can be mentioned the conditions on the ground, footwear, lighting, objects scattered on the ground, among others14,24.
With respect to subjective aspects, it is highlighted the influence of cultural issues involving values and beliefs of the individual, with active effect in the decision-making process. Thus, continuous actions of positive attitudes aimed at preventing certain aspect that can also be stimulated4,20.
Therefore, it mentions the importance of the provision of guidelines and recommendations of health professionals with regard to correct that preventive measures that should be implemented14,16. It's worth mentioning the importance of social networks as friends and family, which can encourage and assist in carrying out the activities21.
About the attributes, antecedents and consequences Prevention Behavior concept, helps its understanding and it was able to find several aspects involved with the theme, as shown in Figure 3.
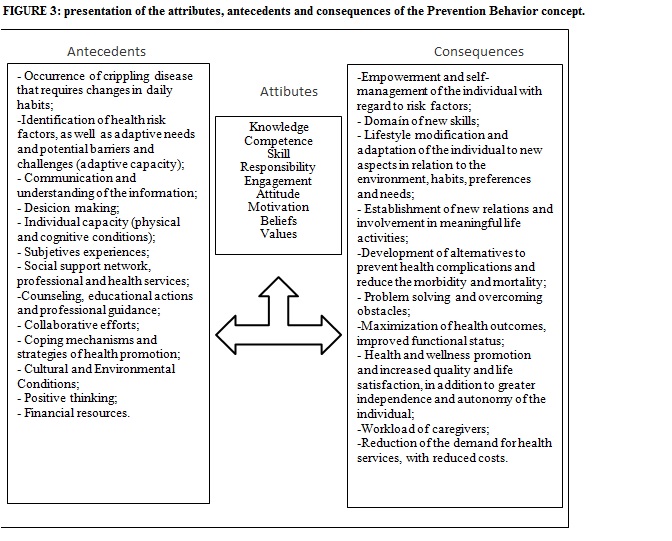
Thus, as verified, prevention behavior has interrelated attributes, employed at the same time, which mentioned skill for the management of individual and environmental conditions3,4,7,8,23-27.
The attribute knowledge was then, the most mentioned in the studies examined1-3,21-24,13-19. There are also other essential attributes to capture the concept phenomenon, as the motivation of the individual who is related to the posture of engagement and previously involved with values and beliefs4,7,20. The last denote the relationship of cultural issue on incorporation of the behavior23.
Knowledge was the more attribute found in the studies and stands out to be closely related to the ability that acquired by knowledge of the subject, with a view to the acquisition of sufficient competence to carry out preventive practices.
However, skill, knowledge and competence are also influenced by an individual's motivation to engage in preventive attitudes1,2,9,13,27, considering aspects of the beliefs and values of the individual4,7,20, since the cultural issue is intrinsically related to the behavior of the individual.
In this context, it mentions the figure of health professionals in the orientation of people as the correct management of risk factors, considering limitations and capacities of the individual1,2,7,8,14-19,21,24,25,27. Moreover, in most of these situations, it is essential that the training of professionals to work with this population, since stroke is one public health problem increasingly common28.
Regarding the antecedents of the concept, it was found that the occurrence of a chronic disease like STROKE, it is often the starting point for the individual to realize the need for changes in certain aspects of life4,19,26 The patient support network also stands to precede and be important driver of the conceptualized event1,2,7,8,14-19,21,24,27. In addition, subjective experiences of the person also are configured as antecedents and are responsible for stimulating preventive behavior9,24.
The antecedent support network can directly influence a person's decision making regarding the prevention behavior21,24. Thus, stimulate collaborative efforts12,15, weighing financial resources, since changes in routine habits involve onus19,23,22.
The subjective experiences are knowledge obtained empirically. In this context, successful experiences influence the individual to believe and trust prevention behavior actions previously experienced and in which benefits were observed.
Through the empowerment acquired the patient experiences significant and positive changes in his lifestyle3,7,9,14,20,21,23,24,26. This process seeks to adapt the person to new aspects imposed by a chronic disease, among which may be mentioned environmental modifications, habits, preferences and needs7,9,21,23,24,26.
With respect to consequences extracted in the search, it has been that after the implementation of preventive behavior, the individual acquires empowerment necessary for the management of the risk factors of the most correct way possible3,14,20. What happens with the intention of establishing alternatives to prevent health complications for the domain of new skills20,22,23.
Therefore, it is highlighted, consequences features of the concept phenomenon, such as: Optimizing functional status, with increased autonomy, and improvement in quality of life26,27.
However, in the context of the patient affected by stroke, it is worth mentioning the phenomenon consequent workload, most commonly experienced by their caregivers who take actions that the patient is unable due to some physical or cognitive sequel21,23. The consequent workload is commonly found in reality of people who experience stroke event, especially in the context of caregivers of patients. The fact is related to the condition of physical dependence that patients with stroke experience and in which caregivers, mostly relatives, ending by putting many of the activities by the patient, overloading him21,23.
In light of the above, it was possible to elaborate a concept that considers the evidence presented and discusses the behavior of prevention as a skill or ability of the individual can acquire. This objective ability to engage in certain activities of preventive nature and employs evidence presented as attributes. It should be noted that, in this engagement, emphasizes the use of preventive strategies with a focus on management of modifiable risk factors leading to preventive actions.
In this way, the process of engagement in the modification or acquisition of new habits culminates in the person's adaptation to changes necessary and often imposed by a chronic disease. The adaptive process experienced is, then, important consequent of the concept studied, as well as obtaining a healthy lifestyle. There are seen to be improving the quality of life another consequence of individual who adopts a preventive behavior.
As the foregoing and based on attributes, antecedents and consequences, it is possible the analysis of concepts from other studies, from which proceeds to the construction of more complete and coherent conceptual definition possible.
In order to formulate the following concept of Preventive Behavior: ability to engage in the management of modifiable risk factors through the use of strategies that facilitate the process of adaptation in search of healthier lifestyle.
CONCLUSION
By reading the papers about the prevention behavior phenomenon, it was possible to identify prevention behavior phenomenon definitions. As well as, several attributes, antecedents and consequences the analysis of these definitions were identified and assisted with a view to elaborate a more completed concept.
It was found that such concepts as being partial definitions of the phenomenon and many other articles not mentioned concepts but attributes, antecedents or consequences. From these recent and based on definitions referred it was possible to elaborate a complete and coherent concept.
Thus, it was possible to clarify the constituent elements of the concept approached, verifying the intrinsic relationship of these. Thus, prevention behavior encompasses aspects of knowledge about risk factors, so that it can be identified them when present. Through collaborative efforts which highlight the role of family members and health professionals, the individual can acquire competence and ability to correct management of risk factors. Finally, we seek to achieve a process of adaptation and incorporation of new habits that can lead to better quality of life.
The conceptual formulation may contribute to better understanding of the professionals who, in turn, can act in a more targeted and individualized, given that the performance of these professionals has been identified as an important antecedent to the phenomenon studied.
It is concluded that the identification of attributes, antecedents and consequences is important because it made possible the clarification of a concept, therefore, greater understanding of the progresses elements, as well as subsequent to the event. Such clarification has demonstrated the benefits that the incorporation of preventive behavior may entail.
REFERENCES
1. Green T, Haley E, Eliasziw M, Hoyte K. Education in stroke prevention: efficacy of an educational counselling intervention to increase knowledge in stroke survivors. Can J Neurosc Nurs. 2007; 29:13-20.
2. Ruffin MT, Nease DE, Sen A, Pace WD, Wang C, Acheson LS, et al. Effect of preventive messages tailored to family history on health behaviors: the family healthware impact trial. Ann Fam Med. 2011; 9:3-11.
3. Wolfe CDA, Redfern J, Rudd AG, Grieve AP, Heuschmann PU, Mckevitt C. Cluster randomized controlled trial of a patient and general practitioner intervention to improve the management of multiple risk factors after stroke: stop stroke. Stroke. 2010; 41:2470-6.
4. Lynch EB, Butt Z, Heinemann A, Victorson D, Nowinski CJ, Perez L, Cella DA. qualitative study of quality of life after stroke: the importance of social relationships. J Rehabil Med. 2008; 40:518-23.
5. Wilson J. Pensar com conceitos. 2ª ed. São Paulo: Martins Fontes; 2005.
6. Walker LO, Avant KC. Strategies for theory construction in nursing. 4th ed. Upper Saddle River, NJ: Prentice Hall; 2005.
7. Gustafsson K, Andersson I, Andersson J, Fjellström C, Sidenvall B. Older women’s perceptions of independence versus dependence in food-related work. Public Health Nurs. 2003; 20:237-47.
8. Astrom M, Asplund K, Astrom T. Psychosocial function and life satisfaction after stroke. Stroke. 1992; 23:527-31.
9. Johansson AEM, Johansson U. Relatives’ experiences of family members’ eating difficulties. Scand J Occup Ther. 2009; 16:25-32.
10. Antle BJ, Mills W, Steele C, Kalnins I, Rossen B. An exploratory study of parents’ approaches to health promotion in families of adolescents with physical disabilities.Child Care Health Dev. 2007; 34:185-93.
11. Redfern J, McKevitt C, Dundas R, Rudd AG, Wolfe CDA. Behavioral risk factor prevalence and lifestyle change after stroke a prospective study. Stroke. 2000; 31:1877-81.
12. Hahn RA, Heath GW, Chang M. Cardiovascular Disease Risk Factors and Preventive Practices Among Adults — United States, 1994. Centers for disease control and prevention. CDC Surveillance Summaries. MMWR, 1998; 47(SS-5).
13. Chan YY, Nagurka N, Richardson LD, Zaets SB, Brimacombe MB, Levine SR. Effectiveness of stroke education in the emergency department waiting room. Journal of Stroke and Cerebrovascular Diseases, 2010; 19:209-215.
14. Redfern J, Rudd AD, Wolfe CDA, McKevitt C. Stop stroke: development of na innovative intervention to improve risk fator management after stroke. Patient Educ Couns. 2008; 72:201-9.
15. Schmid AA, Butterbaugh L, Egolf C, Richards V, Williams L. Prevention of secondary stroke in VA: Role of occupational therapists and physical therapists. J Rehabil Res Dev. 2008; 45:1019-26.
16. Greenlund KJ, Giles WH, Keenan NL, Croft JB, Mensah GA. Physician advice, patient actions, and health-related quality of life in secondary prevention of stroke through diet and exercise. Stroke. 2002; 33:565-71.
17. Kelly-Hayes M. Influence of age and health behaviors on stroke risk: lessons from longitudinal studies. J Am Geriatr Soc. 2010; 58:325-8.
18. Divani AA, Vazquez G, Barrett AM, Asadollahi M, Luft AR. Risk factors associated with injury attributable to falling among elderly population with history of stroke. Stroke, 2009; 40:3286-92.
19. Kann L, Warren CW, Harris WA, Collins JL, Williams BI, Ross JG, Kolbe LJ. Youth risk behavior surveillance - United States, 1995. J Sch Health, 1996; 66:365-77.
20. Levin T, Scott BM, Borders B, Hart K, Lee J, Decanini A. Aphasia talks: photography as a means of communication, self-expression, and empowerment in persons with aphasia. Top Stroke Rehabil. 2007; 14:72-84.
21. Erikson A, Park M, Tham K. Belonging: a qualitative, longitud inal stud y of what matters for persons after stroke during one year of rehabilitation. J Rehabil Med. 2010; 42:831-8.
22. Salter K, Helings C, Foley N, Teasell R. The experience of living with stroke: a qualitative meta-synthesis. J Rehabil Med. 2008; 40:595-602.
23. King RB, Hartke RJ, Houle TT. Patterns of relationships between background characteristics, coping and stroke caregiver outcomes. Top Stroke Rehabil. 2010; 17:308-17.
24. Häggström A, Lund ML. The complexity of participation in daily life: a qualitative study of the experiences of persons with acquired brain injury. J Rehabil Med. 2008; 40:89-95.
25. Desrosiers J, Demers L, Robichaud L, Vincent C, Belleville S, Ska B. Short-term changes in and Neurorehabilitation and Neural Repair, 2008; 22:288-97.
26. Rittman M, Faircloth C, Boylstein C, Gubrium JF, Williams C, Puymbroeck MV et al. The experience of time in the transition from hospital to home following stroke. J Rehabil Res Dev. 2004; 41:259-68.
27. Rabelo DF, Néri AL. Bem-estar subjetivo e senso de ajustamento psicológico em idosos que sofreram acidente vascular cerebral: uma revisão. Est Psicol. 2006; 11:169-77.
28. Oliveira ARS, Costa AGS, Sousa VEC, Moreira RP, Araujo TL, Lopes MVO, Galvão MTG. Condutas para a prevenção de quedas de pacientes com acidente vascular encefálico. Rev enferm UERJ. 2011; 19:107-13.