RESEARCH ARTICLES
Tuberculosis in the family context: experience of family members and patients affected by the disease
Juliane de Almeida CrispimI; Regina Célia FioratiII; Ana Angélica Rêgo de QueirozIII; Ione Carvalho PintoIV; Pedro Fredemir PalhaV; Ricardo Alexandre ArcêncioVI
IRN. Ph.D. candidate and M.Sc. in Sciences, Graduate Program in Public Health Nursing, University of São Paulo at Ribeirão Preto College of Nursing. Ribeirão Preto, São Paulo, Brazil. E-mail: julianecrisp@gmail.com.
IIOccupational therapist. Ph.D. in Sciences, Graduate Program in Public Health Nursing, University of São Paulo at Ribeirão Preto College of Nursing. Ribeirão Preto, São Paulo, Brazil. E-mail: reginafiorati@yahoo.com.br.
IIIRN. M.Sc. in Nursing, Universidade Federal do Rio Grande do Norte. Researcher, Epidemiological-Operational Study Group in Tuberculosis. Ribeirão Preto, São Paulo, Brazil. E-mail: aninha_arego@hotmail.com.
IVRN. Associate Professor, Maternal-Infant and Public Health Nursing Department, University of São Paulo at Ribeirão Preto College of Nursing. Researcher, Epidemiological-Operational Study Group in Tuberculosis. Ribeirão Preto, São Paulo, Brazil. E-mail: ionecarv@eerp.usp.br.
VRN. Associate Professor, Maternal-Infant and Public Health Nursing Department, University of São Paulo at Ribeirão Preto College of Nursing. Researcher, Epidemiological-Operational Study Group in Tuberculosis. Ribeirão Preto, São Paulo, Brazil. E-mail: palha@eerp.usp.br.
VIRN. Associate Professor, Maternal-Infant and Public Health Nursing Department, University of São Paulo at Ribeirão Preto College of Nursing. Researcher, Epidemiological-Operational Study Group in Tuberculosis. Ribeirão Preto, São Paulo, Brazil. E-mail: ricardo@eerp.usp.br.
ABSTRACT: This study aimed at investigating the meaning of tuberculosis to relatives and patients affected by the disease, its impact on family, and the therapeutic resources those actors considered when facing the disease. With qualitative approach, this research involved two relatives and two patients diagnosed at a health unit in Ribeirão Preto, São Paulo, Brazil. Data were collected in 2011 through the focus group technique and analyzed in the light of dialectical hermeneutics. Regarding tuberculosis, relatives and patients display a different rationality from that established by the technical-scientific model. In the family relation, attitudes of distancing and segregating the patient stand out. The subjects consider alternative therapeutic resources to cure the disease. Changes are needed to strengthen the relation between health professionals and family, based on a dialogical process that can acknowledge the family institution as part of TB patient care.
Keywords: Knowledge; family; social stigma; tuberculosis.
INTRODUCTION
The family is the first stage of care and a source of help for people suffering from tuberculosis (TB). According to the author1, the family is the unit where the major determinants of morbidity and mortality in the different age groups are built and operate, either positively or negatively.
People, whilst reflecting about their illness and making decisions, do not act alone but as part of the micro structure (family), which would be more important in the definition of representations and practices related to their health/illness process1,2. Besides, when coping with the illness, each family reacts in a particular way and the situation can be interpreted according to a perception that is determined by the culture and rules established by the society3.
According to the authors3, this context influences the behavior and the relationship among its members when facing the illness. It can be noted that people initially see the situation as a source of stress, and subsequently seek their own possibilities and coping mechanisms4.
In relation to TB, as well as to other infectious diseases, this process is full of contradictions and shows feelings of helplessness, fear and guilt and, at the same time, of overcoming and hope for the cure5. From this perspective, research shows that, in the relationship with society, the stereotyped view of the ill prevails, giving rise to the tuberculosis stigma process6-9.
Although Brazilian literature is rare in relation to the daily contact with the family, research highlights small changes, such as the separation of household utensils and personal objects10,11. This behavior is seen by the authors as a dialectical situation, that is, in the desire of the family to help the sick person, there is still the non-intentional stigma, which is associated with existing beliefs and values12.
In an attempt to understand the complexity involved in the daily life of families and patients with tuberculosis, this study was aimed at investigating the significance of the disease to families and patients, its impact on the families and the therapeutic resources considered by these people when coping with the disease.
THEORETICAL FRAMEWORK
The Dialectic Hermeneutics based on Jürgen Habermas’ perspective was adopted as the theoretical framework of this study13. The trajectory the author points out relates to the theory of communicative action as a possibility for data interpretation, as it brings the dialogical and communicative process as a privileged way of access to the rationality and the understanding about people’s universe of meanings in view of the disease. This is not limited to a mere description of an event but also permits, through language and interpersonal relations involved in communication based on the mutual, reciprocal and coercion-free process, understanding the perceptions of families and TB patients about the disease13,14.
The Habermasian reflection is based on a critique of positivism as a theoretical framework of modernity, which leads to the eradication of the subject, the intersubjectivity, the values, the rules, the history, the knowledge to give way to a mathematized, objective, universal and superficial interpretation of the world. Accordingly, it uses a deeper analysis that proposes the submission of the instrumental to the communicative rationality, and the reestablishment of the democratic activity, based on the construction of consensus founded and supported on the dialogical and intersubjectivity of the subjects, as a way to coordinate the social and human practice15.
According to the author, when pointing out the language as a way of accessing thoughts, knowledge of the reality and the human social universe, the interpretation of reality and human relations through the intersubjective rationale is raised and, therefore, no longer monological, but rather dialogical. Thus, the human interaction is a process by which people find solutions to their problems and coordinate among themselves in order to create and put their plans of action into practice as social actors in the field of negotiations and possibilities13.
In the human interaction, there are two different dimensions: the communicative and the strategic acting, which are both linguistically mediated; however, the strategic acting is aimed at a teleological action with determined purposes for practical success and, with that intent, the language is used as a way of information. On the other hand, the communicative acting aims at the mutual understanding between people about a certain reality and, therefore, the use of language is focused on the understanding of both and it requires cooperation in coordinating their plans of action, demanding the use of the shared language16. From this, men and women have the communicative acting as a basic tool to understand any reality or event. Based on a dialogical and intersubjective process, everyone involved in this interaction must have the same values. Thus, it is believed that the adoption of this framework in the study helps to understand the complexity involved in the daily lives of families and patients with TB.
METHOD
This is a descriptive study with a qualitative approach, undertaken at a Referral Center for Diagnosis and Treatment of Tuberculosis located in the city of Ribeirão Preto, in the state of São Paulo, Brazil. In this town, the care provided to people with TB is centralized in the reference outpatient care centers, which are distributed into five secondary healthcare units with Tuberculosis Control Program (TCP), providing specialized teams and performing actions directed at the diagnosis and medical management of cases and their communicators.
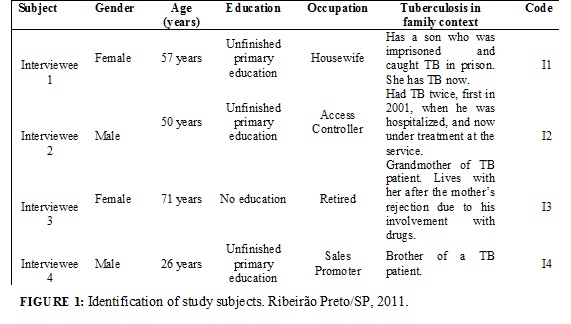
In this Referral Center, the invitation to participate in the study was extended to twenty patients and their family members – communicators of TB patients who were diagnosed in the period between January and June 2011. However, only four people (two relatives and two family members) met the inclusion and exclusion criteria, as per Figure 1. The inclusion criteria involved people from both genders who lived with the TB patients, over 18 years of age, who agreed to voluntarily participate in the research and were available to travel to the healthcare unit, with funds offered for transportation. The exclusion criteria involved people under 18 who did not agree to participate in the research.
Data collection took place in May 2011 through the focus group technique, which lasted for one hour and 15 minutes. This technique was chosen because the event under investigation has an ideological and perceptive nature, resulting from the cultural movements and the symbolical dimension of the human experience. Such technique, while enabling group interaction, helps the redevelopment of their own values, judgments and opinions about the researched object based on a dialogical and intersubjective construction, permitting a collective knowledge production17. The group discussion was conducted by a facilitator, following a previously prepared guide with the following guiding questions: What is TB? Has the TB caused changes in your family relationship? What do you think about the TB treatment?
Data analysis was performed based on dialectical hermeneutics, which allows the interpretation of reality as an investigation of significance through a linguistic or thematic analysis18. Initially, data collation was performed through the reading and rereading of the transcribed material and subsequently, the researchers identified the convergent points, themes, subjects, approaches or relations that were shared in the several statements of the people, based on an interpretative process of such information.
The development of the study met the ethical principles of Resolution number 466/2012 of the National Health Council, and the Research Project received approval from the Research Ethics Committee at the University of Sao Paulo at Ribeirão Preto College of Nursing (Decision 1292/2011). The request for participation in the study was verbal and followed by the Informed Consent Form. The participants were informed about the objectives and the data collection technique and, in order to ensure their anonymity and, among other aspects, the preservation of their identities in presenting the results, the statements of the participants were identified by the letter I (interviewee), followed by the number of the study participant.
RESULTS AND DISCUSSION
Through data analysis, three categories emerged: the significance of TB in the context of the families: gap between knowledge and the technical and scientific knowledge; the disease’s impact in the family relationship; and TB and the alternative therapeutic resources existing in the communities.
The significance of tuberculosis within the family context: gap between knowledge and the technical and scientific knowledge
When referring to what tuberculosis is, families and patients show a rationale that differs from the knowledge established by the technical and scientific model. The subjects involved see TB as a transmissible and curable disease, caused by the lifestyle and which presents itself in such a scary way that an interviewee hesitated to pronounce the word tuberculosis, using the term dangerous disease when referring to it.
It is a lung infection, something like that. It is a transmissible disease, I know this. Every time I go to the public health care center, I always read: who has a cough for more than three weeks […] should look for a hospital to check whether they have tuberculosis or not. It can be cured, I know this. (I1)
I would like to know, some say it is due to bad nutrition […], with me, it has been repeating, I went through a treatment in 2001 and now it is back. They say it is due to bad nutrition, who crosses the line and all, mine is due to this. (EI2)
What he is saying is true, there are people who say something, other people say something else. They say it is coldness, malnutrition […], I think it is a dangerous disease, I want to know if it is contagious […]. I would like to know because I have my grandson in my house. (I3)
It can be noted in the statements of the interviewees that the view about the TB is not due to a lack of information, but the need to turn such information into operationalized knowledge in the context of families.
According to Habermas’ dialectical hermeneutic framework16, the sphere of human condition, of interaction guided by the communicative rationality, based on the intersubjectivity and aimed at mutual understanding through which people take a stand according to their political-ideological projects and plans of action, should guide the instrumental sphere in order to ensure that the knowledge of families in relation to the TB are shared and discussed in the face of strictly technical and biological interests relating to the disease.
Regarding the current health care practices, there is large investment in the training of healthcare professionals in order to successfully respond to the technique, but there is no concern in relation to the incorporation of devices that encourage the interaction and sharing for the construction of singular therapeutic projects. Most of the time, the technical and scientific discourse of the healthcare professionals overcomes the discourse of users, taking away its legitimacy and validation and their condition of users who have a discourse in relation to their own interpretation of experiences based on their sociocultural universe19.
In this context, care should consist of a relationship among team, family and patient, in so far as it proposes the improvement of the health condition and quality of life of all the people involved. Therefore, the work of professionals cannot be limited to the technical activities but should rather consider the exchange between different knowledge and the existing technical and scientific knowledge in order to provide a safe and an ethical interpersonal relationship11,20.
The disease’s impact on the family relationship
The occurrence of the disease affects the sick persons and their entire family dynamics, bringing the crisis experience that activates a series of responses and behaviors, due to the uncertainties caused by the damaged health21.
In this study, patients report changes that occurred in the interaction with the family and the society after the diagnosis – according to the statement below:
The first time I had it (TB), my sister burned all my things, even the blanket […] then she started to separate everything. It has been five years since I had contact with them. This time, my wife has separated my things from the boy’s […]. In the place she works at, the boss was going to sack her from her job because of my disease, because she is living with me […]. (I2)
Because we know that tuberculosis is similar to leprosy, which is not caught and is not transmissible, but everyone starts to keep away from the sick people. (I1)
The people infected, while coping with the illness, experience a large emotional impact, marked by isolation in their relationships both within and outside the family6,8. It can be noted that the interviewees show fear and sadness, and are under the impression that everyone around views them as different people and they blame themselves for their situation.
There was no change in the statement of the family, and the separation of objects is marked by the ambivalence between caring for the other and the remaining non-intentional stigma. Throughout the centuries, the negative representations about the TB have spread and still remain in modern society22.
At home, nothing has changed, he is sleeping in the living room because the back room is too stuffed […], he was very thin and could not climb up on the bunker bed, so we opted for the living room, where we open the windows […]. I’ve also separated my grandson’s clothes and cup, it is all separated. (I3)
Despite this ambivalence, a study shows that the families are concerned with the influence of the discrimination on their sick family member; therefore, to openly speak about TB in the community and in the healthcare services where the sick people undertake treatment becomes a complex and challenging issue, which can stop them from having the support and help from their social relationships23.
This situation indicates the need for effective actions concerning guidelines for the TB. However, it is highlighted that these actions should go through a re-signification process, in which the political commitment of managers and healthcare professionals should be sensitive to the social relations within families, in order to include them in the care plan of TB patients. Therefore, the work of a multiprofessional team that is sensitive to the problem and discusses the possibilities of interventions from the biological to the social aspect of the disease becomes relevant.
Every communicative action becomes effective when it is based on the awareness and mutual understanding of people about something13, being the equality of chances in relation to the dialogued statements essential for the construction of consensus and end of stigma concerning the TB. It is therefore necessary to establish a dialogical and intersubjective process within the family and the healthcare teams’ dynamics.
Tuberculosis and the alternative therapeutic resources existing in the communities
The therapy based on the traditional practice of medicine is an aspect that is present in the Brazilian society. In certain contexts, such condition is based on the culture, historical and social values of the different communities. This category is shown by the following statement.
If they (the patient) had gone straight to my house, they would have gone to the public healthcare center, I would have prepared a home-made medication, because I have never heard of this disease, I thought it was the flu, a cold […] I would have prepared a home-made medication and given them a pill. (I1)
The lack of knowledge about the TB, the association with the flu and the use of home-made medication can be explained by the beliefs and popular knowledge of the interviewees when coping with the disease. Therefore, in this statement, the importance of educational healthcare strategies can be noted, which take into consideration the beliefs, the popular knowledge and the alternative therapeutic resources existing in the community, trying not to assume that the people involved do not have any knowledge about TB, but critically reflect whether the healthcare professionals are able to direct them, taking into account their understandings5.
Based on this, the strictly biomedical framework is not sufficient to have access to the understanding about the issues involving families and TB patients. In order to experience them as a constitutive element of the human condition, it is imperative to establish a dialogue between the various alternative systems for the construction of healthcare models with social credibility, taking into account that the separation between the healthcare sector and the other alternative systems tends to contribute to the eradication of TB in the communities24.
CONCLUSION
The cognitive contents of the statements showed that the significance of the TB to families and patients has a rationale that differs from the knowledge instituted by the technical and scientific model. TB affects not only the sick person but also their entire family dynamics. It is noted that patients experience an emotional impact, marked by isolation in their social relationships, and that families experience the ambivalence between taking care of them and the existing stigma. The beliefs and popular knowledge encourage the search for alternative therapeutic resources for coping with the disease.
The authors highlight, as limitations of this study, the losses related to the participation of patients and the difficulty to openly speak about the disease in its context. However, from a universe of four people, important aspects affecting the therapeutic and life projects of family members and TB patients could be revealed. The study, involving only four people, does not allow the generalization of its findings.
It is imperative to reflect about the importance of the family in the life course of patients with TB as a social institution and the need to recognize it as a support and an intervention network in the definition of policies directed at TB control.
REFERENCES
1. Menéndez E. Grupo doméstico y proceso salud/enfermedad/atención. Del teoricismo al movimento continuo. Cuadernos Médico Sociales. 1992; 59: 3-18.
2. Leite SN, Vasconsellos MPC. Negociando fronteiras entre culturas, doença e tratamento no cotidiano familiar. Hist cienc saúde-Manguinhos. 2006; 13:113-28.
3. Sousa AS, Kantorski LP, Bielemann VLM. A Aids no interior da família – percepção, silêncio e segredo na convivência social. Acta Sci Health Sci. 2004; 26:1-9.
4. Suit D, Pereira ME. Vivência de estigma e enfrentamento em pessoas que convivem com o HIV. Psicol USP. 2008; 19:317-40.
5. Rodrigues ILA, Souza MJ. Representações sociais de clientes sobre a tuberculose: desvendar para melhor cuidar. Esc Anna Nery. 2005; 9:80-7.
6. Baral SC, Deepak KK, Newell JN. Causes of stigma and discrimination associated with tuberculosis in Nepal: a qualitative study. BMC Public Health. 2007 [cited in 2011 Jul 25] 7:211. Avalaible in: http://www.biomedcentral.com/1471-2458/7/211.
7. Somma D, Thomas BE, Karim F, Kemp J, Arias N, Gosoniu GD, Abouihia A, Weiss MG. Gender and socio-cultural determinants of TB-related stigma in Bangladesh, India, Malawi and Colombia. Int J Tuberc Lung Dis. 2008; 12:856-66.
8. Dodor EA, Kelly S. We are afraid of them’: Attitudes and behaviours of community members towards tuberculosis in Ghana and implications for TB control efforts. Psychol Health Med. 2009; 14:170-9.
9. Atre S, Kudale A, Morankar S, Gosoniu D, Weiss MG. Gender and community views of stigma and tuberculosis in rural Maharashtra, India. Glob Public Health. 2011; 6:56-71.
10. Clementino FS, Martiniano MS, Clementino, MJSM, Sousa JC, Marcolino EC, Miranda FAN. Tuberculose: desvendando conflitos pessoais e sociais. Rev enferm UERJ. 2011; 19:638-43.
11. Freitas IM, Crispim JA, Pinto IC, Villa TCS, Brunello MEF, Pinto PFPS, Arcêncio RA. Conhecimento e percepção sobre tuberculose das famílias de pacientes em tratamento diretamente observado em um serviço de saúde de Ribeirão Preto-SP, Brasil. Texto contexto – enferm. 2012; 21:642-9.
12. Macq J, Solis A, Martinez G, Martiny P, Dujardin B. An exploration of the social stigma of tuberculosis in five “municipios” of Nicaragua to reflect on local interventions. Health Policy. 2005; 74:205-17.
13. Habermas J. Teoría de la acción comunicativa. Madrid (Es): Taurus; 1988.
14. Fiorati RC, Saeki T. A inserção da reabilitação psicossocial nos serviços extra-hospitalares de saúde mental: o conflito entre racionalidade instrumental e racionalidade prática. Rev ter ocup USP. 2011; 22:76-84.
15. Fiorati RC, Saeki T. As atividades terapêuticas em dois serviços extra-hospitalares de saúde mental: a inserção das ações psicossociais. Cad Ter Ocup UFSCar. 2012; 20:207-15.
16. Habermas J. Teoría de la acción comunicativa: complementos y estúdios prévios. Madrid (Es): Ediciones Cátedra; 1994.
17. Gatti BA. Grupo focal na pesquisa em ciências sociais e humanas. Brasília (DF): Líber Livro; 2005.
18. Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. São Paulo: Hucitec; 1992.
19. Ayres JRCM. O cuidado, os modos de ser (do) humano e as práticas de saúde. Saude soc. 2004; 3:16-29.
20. Formozo GA, Oliveira DC, Costa TL, Gomes AMT. As relações interpessoais no cuidado em saúde: uma aproximação ao problema. Rev enferm UERJ. 2012; 20:124-7.
21. Milioni DB, Sanchez KOL, Nunes MDR, Filizola CLA, Ferreira NMLA, Dupas G, et al. Enfermagem familiar: o conhecimento produzido para além das fronteiras nacionais. Rev enferm UERJ. 2011; 19:650-6.
22. Pôrto A. Representações sociais da tuberculose: estigma e preconceito. Rev Saude Publica. 2007; 41:43-9.
23. Johansson E, Long NH, Diwan VK, Winkvist A. Attitudes to compliance with tuberculosis treatment among women and men in Vietnam. Int J Tuberc Lung Dis. 1999; 3:862-8.
24. Tesser CD, Barros NF. Medicalização social e medicina alternativa e complementar: pluralização terapêutica do Sistema Único de Saúde. Rev Saude Publica. 2008; 42:914-20.