RESEARCH ARTICLES
Falls occurrence and body mass index in elderly
Alice Gabrielle de Sousa CostaI; Francisca Bertília Chaves CostaII; Ana Railka de Souza OliveiraIII; Viviane Martins da SilvaIV; Thelma Leite de AraujoV
INurse. Doctorate in Nursing by the Federal University of Ceará. Scholarschip of the Cearense Foundation of Scientific and Technologic Support and
Development. Fortaleza, Ceará,Brazil. E-mail: alice_gabrielle@yahoo.com.br
IINurse. Master in Nursing. Nurse of Family Health Strategy. Fortaleza, Ceará, Brazil. E-mail: bertilia.chaves@hotmail.com
IIINurse. Doctorate in Nursing by the Federal University of Ceará. Scholarship of the Cordination of Personnel Improvement of High Education. Fortaleza,
Ceará,Brazil. E-mail: railkaufc@yahoo.com.br
IVNurse. Doctorate in Nursing. Professor of the Gradation and Post-Graduation course in Nursing of the Federal University of Ceará. Fortaleza, Ceará,Brazil.
E-mail:vivianemartinsdasilva@hotmail.com
VNurse. Doctorate in Nursing. Professor of the Graduation and Post-graduation course in Nursing of the Federal University of Ceará. Fortaleza, Ceará,Brazil.
E-mail: thelmaaraujo2003@yahoo.com.br
ABSTRACT
The study aimed to compare four groups of elderly with and without stroke and falls. A case-control study that was performed in Fortaleza city, 2010.Data collected by interview through a form that evaluated demographic variables, health status and body mass index in 60 elderly. Most of the groups were composed by women (66.7%), mean age of 69.86 to 71 years. Those who had suffered a stroke had presented an average of 1.4 events (±0.67) at a time of 5.6 years (±7.5). The number of stroke was slightly higher (1.4 ±0.63) at the groups with fall history. The majority reported a regular health condition and was overweight or obese. This way, the risk factors for falls should be continuously evaluated by qualified professionals, in order to maintain favorable conditions for elderly health.
Keywords: Eldery; accidental falls; body mass index; stroke.
INTRODUCTION
The occurrence of fall configures itself as one of the main aggravations of health evidenced in elderly individuals who experience physical changes inherent in the physiological process of aging1.
Although this event is an event most in old age, it should not be seen as something inherent in this age group. But the risk factors should be continuously evaluated by qualified professionals, in order to maintain favorable health conditions of the elderly.
In this context, the evaluation of the body mass index (BMI), providing a nutritional parameter measurement of individual as well as data on the intrinsic condition that may be favorable to the occurrence of a fall. Thus, the extremes of weight can be identified, enabling the joint prevention mechanisms further.
Thus, the aim of this study was to characterize elderly with or without history of falls as: the social demographic variables, occurrence of the event fall and stroke, health conditions and intrinsic factor BMI.
THEORICAL REFERENTIAL
The fall phenomenon appears as a drop an unintended event that results in the change of position of the individual to a lower level in relation to its initial position1.
Between external causes, the falls highlights by meeting the highest proportion of admissions of females (42.39%) and elderly (57.85%). Taking into account only the metropolitan region of Fortaleza, in 2009, it was verified 3,636 hospitalizations from episodes of falls. Deaths from falls have increased in recent years and 70% of accidental deaths in people with 75 years old were motivated by this event2. It is believed that as the reporting system has become more efficient, the importance of the falls has become even more evident.
The risk factors that lead to the fall event can be multifactorial and involve intrinsic and extrinsic conditions. The term intrinsic factors are those arising from physiological changes possibly related to advancing age. The extrinsic, are related to environmental aspects, such as flooring, lighting conditions and shoes used.
In this context, with reference to the intrinsic factors, the extremes of weight, the excessive thinness or obesity, can be perceived as important falls 3 inductors and calculating the BMI provides a parameter for the evaluation of such extremes.
It has been shown that the postural imbalance, in terms of overweight and obesity, can be one of the causes of falls during the daily activities of the elderly, once the obese have less range of motion, that is, they are stricter. The study points out that to restore the balance is required a greater torque on the ankle joint, due to the accumulation of fat in the abdominal area4.
Unintentional weight loss is also an important indicator for the realization of weakness in the elderly5. This phenomenon is also related to fatigue, weakness and competes for the increase in inactivity and physical dependence, factors that contribute significantly to the occurrence of falls, in addition to raising the number of hospitalizations and institutionalizations6,7.
The study found that 40% of elderly were overweight or obese. Elderly obese, may have compromised balance by greater physical condition and uneven from the aging and, thus, the risk of falling is increased8.
These physiological changes of aging when added to the consequences of disabling diseases such as stroke (CVA) can greatly increase the chances of happening falls, given the possibility of sequels that interfere with gait and balance9.
In this context, it is stressed that the measure of weight and BMI calculation is a method of low cost, easy implementation and providing a significant accuracy to estimate body fat and health assessment.
From the point of view of health care, it is recommended that early identification and correct the main risk factors for falls can converge to the possibility of preventing this interlocutory appeal, avoiding the numerous complications that a fall can cause10.
METHODOLOGY
It Is a study of case-control type in which it considered the occurrence of falls as outcome variable. In order to reduce biases, the 60 participants were assembled in four groups, with 15 elderly each. Of these, one was a case group, named GCA (elderly with stroke that fell) and three groups controls, GCO1 (elderly with stroke that didn't fall), GCO2 (elderly without stroke that fell) and CGO3 (elderly without stroke that didn't fall), taking as a base the last fall during the last six months.
The locations of the study were three Charitable Associations Rehabilitation of Ceará (ABCR) and a Center of Reference of Social Assistance (CRAS), all located in Fortaleza, Ceará. Data collection was operationalized in the months of January to April 2010.
Because it is a study of case-control type and the inadequacy of records of the research locus units the sample could not be estimated in advance. We decided, then, by selecting all those individuals who frame the inclusion criteria: to be registered in the unit collects, having age over 60 years and have experienced event of stroke with medical diagnosis confirmed. In groups composed of individuals with falls, this should have occurred in more than six months. Exclusion criteria of the study were: individuals who do not submit conditions to stand even with use of aid device, such as a cane or people with cognitive deficit, characterized by inability to understand a command and establish verbal communication.
The data were collected through an interview and through a structured form submitted the test with six elderly, which investigated social demographic data, health conditions and anthropometric measurements (weight and height). For measurement of the latter, it was used the following equipment: anthropometric scale properly tested and calibrated Future Plenna Digital brand, with a capacity of 150 kilograms (kg) and precision of 100 grams (g), inelastic tape measure, with a capacity of 1.5 meter (m) and sensitivity of 0.5 centimeter (cm).
Weight measurements were made with the participant in orthostatic position, positioned in the center of the scale with feet together and arms stretched along the body. It was found the stature through the measuring tape affixed to one wall and the participant maintained in standing position, bare feet and united, pending arms, hands flat on the thighs and chin upright.
About the BMI, it was obtained by dividing the body weight in kilograms by the height in meter high squared (kg/m2). For classification of values it was adopted the recommendation of the Ministry of Health11 for evaluation of adults and older people: below normal (BMI < 18.5), normal (BMI of 18.5 to 24.9), overweight (BMI of 25 to 29.9), obesity I (BMI of 30 to 34.9), obesity II (BMI of 35 to 39.9) and obesity III (BMI ≥ 40) III.
The data were organized into worksheets Excel 2007 program and analyzed by absolute frequencies and percentages. The study was forwarded and reviewed by the Research Ethics Committee of the Federal University of Ceará, being adopted as Protocol No 314/09. In addition, participants received assurances about anonymity and freedom to voluntary participation, without prejudice in attendance in case of refusal. Those who attended the invitation were advised to the signing of an Informed Consent and Clarified Term.
RESULTS AND DISCUSSION
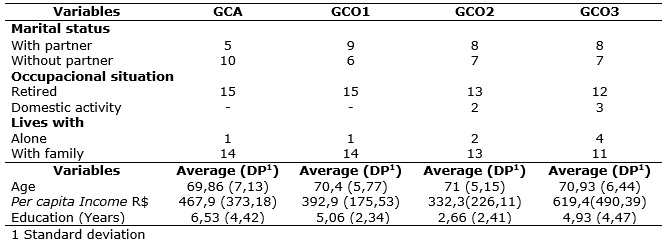
Each study group (GCA, GCO1, and GCO2 GCO3) was composed by 10 (66.7%) women and only 5 (33.3%) men and showed normal distribution, with an average age that ranged from 71 to 69.86 years old among the groups.
The female population was singled out by still other studies as the category most affected by falls12. This fact is due not only to higher life expectancy of women and a greater propensity to fall, but, mainly, to osteoporosis, more pronounced in females13.
In an investigative research on the related factors with the condition of the woman who falls, it was found association between falls and the following variables: absence of extradomiciliary labor activities, suggesting immobility and the decline of its functional capacity; the presence of diabetes, by facilitating the emergence of other Comorbidities, in addition to the own disease disorders; articular diseases, by restricting their functional abilities and sensorineural components changes, which provide amendments to the balance and proprioceptive deficit14.
As the data shows, most of the members of the groups consisted of elderly retirees, who owned partner and resided with relatives. The average per capita income ranged varies from 332.30 to 619.40 reais and education was found in individuals with stroke and fall, with 6.53 (4.42 ±) years of study.
About people who live with, the study found statistical association between the variable to live alone and the possibility of occurrence of fall become something common or chronic (OR: 1.53 [0.97-2.41] p = 0.032). This outcome was also associated with the absence of a partner (OR: 1.57 [1.04-2.37] p = 0.015)14. In this study, however, few elderly reported living alone. It is highlighted that, in all groups, it is found people in this condition, as shown in Table 1.
TABLE 1:
Distribution of participants case groups (GCA) and controls (GENCO) according to the social demographic variable (n=60). Fortaleza, 2010
With respect to participants who have suffered stroke, it was identified an average of 1.4 event of stroke (± 0.67), in an average time of 5.6 years (± 7.5).
As for the groups of individuals who reported falls (GCA and GCO2), the number of events was slightly higher in individuals who had experienced stroke (1.4 ± 0.63) than in others (1.2 ± 0.45). The time since the last occurrence of the fall was also higher in the first group (2.6 months) with respect to the elderly without stroke (1.9 month). Among the elderly with stroke, only five mentioned the occurrence of falls before the disease and of these, four reported falls for at least six months, compounding the case study group (GCA).
It is known that the predisposition of the elderly related to decreased stability can be increased due to the physical consequences caused by stroke, as hemiplegia or hemiparesis, which cause the individual limitations in movements of arms and legs. These limitations become evident during quick walks, when there is a reasonable risk of a fall. In a severe hemiplegia, the knee of the affected limb is maintained in extension and ankle in plantar flexion and slightly inverted. With the movement of the legs in a broad pattern swing, the foot hemiplegic tends to drag on, putting the patient at great risk of falling by stumbling13.
Generally speaking, the falls are frequent at all times of life, especially in the elderly. In these cases, may represent a more serious health problem. It stands out, in this context, the following: elderly individuals, when they fall, are at greater risk of injury. The psychological impact of the falls, constitutes as a deciding factor among older people, and the loss of confidence in the ability to ambulate safely can result in worsening of functional decline, depression and social isolation9.
As regards health conditions of respondents, there were differences between the groups, but overall, the regular condition was the most cited by respondents. It should be noted that in the group without fall and without stroke (GCO3), no elderly mentioned bad health condition or terrible.
Most of the participants of this research showed a regular state of health. Among those who reported a state of optimal health, most belonged to the group of individuals without reports of falls or stroke, and of these, any participant showed bad health or terrible, according to figure 1.
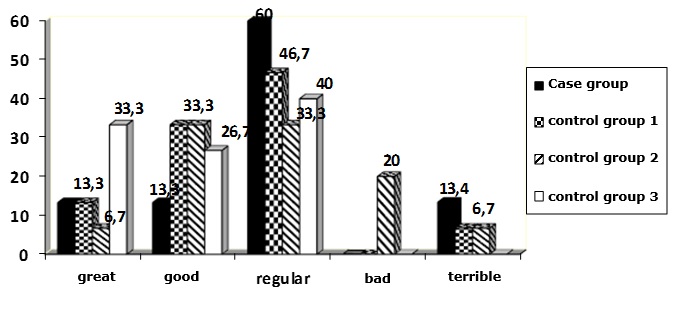
FIGURE 1
: Percentage of individual health conditions according to individual perception of each research group. Fortaleza-CE, 2010.
Various health problems can increase the chances of a fall. The orthostatic hypotension, for example, has been reported with frequency in elderly people, which is associated primarily with the use of drugs13.
It was assessed, yet, the values of BMI of participants in each group, which remained with uniform layout between the groups. It should be noted, however, that more than half of those surveyed were overweight or obese in all study groups. In GCO3, it was also identified an individual in the classification of obesity II and other obesity III, as shown in Table 2.
TABLE 2:
Characterization of the case groups (GCA) and controls (GENCO) study participants according to the body mass index. Fortaleza-CE, 2010. (N=15 per group)
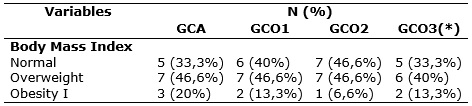
(*)An individual with obesity II and na individual with obesity III were found
It is known that the nutritional status of the aged and his BMI can be related to likely to happen falls. Thus, the extremes as regards the classification of BMI should be carefully evaluated, by inducing the weakness of the individual or even a loss of balance. Obese individuals, for example, usually have a physical structure and greater than the body can withstand, spoiling the balance. This has been amended in consequence of the aging process, and, therefore, when associated with the inadequate nutritional status, accentuates the risk of the elderly fall15.
It is worth mentioning that some changes in anthropometric elderly may be related to physiological changes of that age range, such as reducing the contents of body water and muscle mass, which can contribute to gradual decrease of weight. Change in amount and distribution of the subcutaneous adipose tissue and muscle mass transformation in intramuscular fat can also lead to a mistaken assessment of malnutrition13.
The physiological changes of aging related to weight and body fat distribution end, then to limit the predictive power of anthropometric indicators, such as the BMI. The cases of thinness, however, were related as factors that can make a person more prone to the occurrence of falls3. Weight loss can contribute to the possibility of fragility and is associated with fatigue in the elderly, this was perceived in 15.87% of a population of elderly 5.
Despite the changes that contribute to decrease the weight, it was noticed in the study well prepared that none of the participant was in the classification of low weight, with a predominance of individuals with overweight or obesity. Another study with elderly found similar data, also with a predominance of people obese or overweight, particularly among those who reported physical inactivity, in the other, the practice of water aerobics was the most noticeable and was associated with the best body mass indexes8,16. Thus, in addition to help in the control of BMI, physical exercises are recommended for individuals with fear of falls and increased risk for the event16.
Thereby, a BMI within the bounds of normality, and enable best performance on achievement of everyday movements and make the mobility of the elderly safer, prevents against unexpected injuries that can bring serious limitations for this population16.
Regarding the patients with stroke, it is important to mention the possibility of physical deficits and greater predisposition to inactivity, as well as increasing the degree of dependence of the elderly. Thus, individuals who are overweight or obese grow more difficult the actions taken by caregivers and increase the chances of accidents like falls when the implementation of care.
Due to the overweight of the elderly, activities of caregivers may involve development of complications such as back pain, pain in the lower limbs and fatigue. Caregivers must be addressed, since, in addition to suffer direct consequences for overweight of the familiar, they participate actively in the preparation of food at home17.
As for the average of falls in the last six months found in this study (1.4 ± 0.63 in case group and 1.2 ± 0.45 in the control group), this appeared similar to other research, in which the majority of the elderly fell once or twice during this period3. However, in both groups of elderly falls (GCA, GCO2) it was observed average over a fall per participant. This fact denotes the recurrence of falls in a period of six months.
It should be noted that the average falls was even greater in the group with stroke. In previous research, positive statistical correlation was observed between the occurrence of falls and the stroke event. Most of these patients (67%) reported the occurrence of multiple falls, to denote the importance of identifying the existence of recurrent falls as an additional risk factor18.
The occurrence of falls is therefore a widespread problem among the elderly, that can lead to severe consequences. Of these, the most common is the occurrence of fractures. In the population over 75 years of age, on average, one-third of individuals suffer one or more episodes of fall. This is reported as the most prevalent among the accidents that occurred at home19.
It is noticed that the falls are real events in the lives of elderly and brings serious consequences to them, such as fear of the recurrence of the event, fractures or even death. These events are more damaging not only to the victims but also to those who live with the patient. In addition, the falls represents onus for the health sector and should be seen, definitely as a public health problem8.
Given the above, the major challenge for the Brazilian public health will take care of a large elderly population and females, most with low socioeconomic and educational level. Adequate access to health care, including preventive services, can reduce the morbidities, dependence and mortality, as well as preserving the physical and mental functions, contributing to the increased likelihood of a healthy old age14.
So, innumerous are the risk factors for falls and these represent the leading causes of disability among the elderly. It should be noted that the elements of vulnerability are also related to the social context in which the elderly live, with the changes of health and, often, with impossibility to access to therapeutic resources20.
In this context, most health professionals are not yet prepared to face this reality, whether in the preventive aspects, whether assistance issues following the occurrence of the fall13.
The professional preparation is justified, especially for being a fundamental action to correct and effective identification of risk factors for falls, because to acknowledge them, the professional acquires ability to lay out a plan of actions aimed at prevention of falls. It can then promote the health of clients, with a focus on healthy ageing, optimization of their functional capabilities, and ease the financial burden caused to health services.
In this perspective, the greatest challenge to the Brazilian public health will take care of a large elderly population and females, most with low socioeconomic and educational level. Adequate access to health care, including preventive services, can reduce the morbidities, dependence and mortality, as well as preserving the physical and mental functions, contributing to the increased likelihood of a healthy old age14.
CONCLUSION
Most groups were composed by women, aged 70 years, retirees, residing with relatives and had low per-capita income. Also it was found low education, oscillating from 2.6 to 6.5 years of education. The case group was that showed the highest number of falls in the past six months.
With respect to the intrinsic risk factor BMI changed, there was a uniform layout between the groups. However, the majority of respondents were overweight or obese and this fact was noted in all groups, which denotes the importance of allocating greater attention to this factor that demonstrably is related to the increased risk of falls and that is modifiable and amenable to preventive actions.
Thus, the present study launches a range of opportunities for the development of new research linking the event falls and the intrinsic factor BMI changed mainly in other populations, because early identification and correct the main risk factors for falls converges to the possibility of preventing this interlocutory appeal. The limitations of the study are based on small sample size that reduces the chances of generalization of the findings.
Although the fall is an event more of old age, it should not be seen as something inherent in this age group. But the risk factors should be continuously evaluated by qualified professionals, in order to maintain favorable health conditions of the elderly.
In the context of prevention and health promotion, it is highlighted, yet, the actions of the network of primary health care, with emphasis on the family health strategy, for being involved with the everyday reality of the population and give direct actions in the home setting of the individual. And, in this case, it stands the figure of the nurse as a member of team, able to carry out the management of the main actors involved in health promotion for the elderly, such as the family and social support networks, in order to fix, mitigate or work in an environment conducive to autonomy and quality of life of the elderly.
REFERENCES
1.Fabricio SC, Rodrigues RA, Costa Junior ML. Falls among older adults seen at a Sao Paulo State public hospital: causes and consequences.Rev Saúde Pública. 2004; 38:93-9.
2.Ministério da Saúde (Br), DATASUS. Indicadores de morbidade e fatores de risco. Proporção de internações hospitalares (SUS) por causas externas [site de Internet]. Brasília; 2009 [citado em 1 dez 2010] Disponível em: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?idb2009/d14.def.
3.Lojudice DC. Queda de idosos institucionalizados: ocorrências e fatores associados [dissertação de mestrado]. Ribeirão Preto (SP): Universidade de São Paulo; 2005.
4.Carneiro JAO. Idosos obesos têm mais risco de quedas. Associação Brasileira para o Estudo da Obesidade e da Síndrome Metabólica [site de Internet] 2010. [citado em 7 set 2011] Disponível em: http://www.abeso.org.br/lenoticia/579/idosos-obesos-tem-mais-riscos-de-quedas.shtml .
5.Costa TB, Neri AL. Medidas de atividade física e fragilidade em idosos: dados do FIBRA Campinas, São Paulo, Brasil. Cad Saúde Pública. 2011; 27(8):1537-50.
6.Linck CL, Crossetti MGO. Fragilidade no idoso: o que vem sendo produzido pela enfermagem. Rev Gaúcha Enferm. 2011; 32:385-93.
7.Remor CB, Bós AJG, Werlang MC. Características relacionadas ao perfil de fragilidade no idoso. Sci Med. 2011; 21(3):107-12.
8.Costa AGS, Souza RC, Vitor AF, Araujo TL. Acidentes por quedas em um grupo específico de idosos. RevEletr Enf. 2011; 13:395-404.
9.Freitas EV, Py L, Cançado FAX, Doll J, Gorzoni ML. Distúrbios da postura, marcha e quedas. In: Freitas EV, Py L, Cançado FAX, Doll J, Gorzoni ML. Tratado de geriatria e gerontologia. 2ª ed. Rio de Janeiro: Guanabara Koogan; 2006. p. 950-61.
10.Wada N, Sohmiya M, Shimizu T, Kamoto K, Shirakura K. Clinical analysis of risk factors for falls in home-living stroke patients using functional evaluation tools. ArchPhysMedRehabil. 2007; 88:1601-5.
11.Ministério da Saúde (Br). Vigilância alimentar e nutricional - Sisvan: orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde. Brasília (DF): Ministério da Saúde; 2004.
12.Santos ACS. Valor dos instrumentos de avaliação de risco de quedas em idosos com fibrilação atrial [tese de doutorado]. Ribeirão Preto (SP): Universidade de São Paulo: 2007.
13.Ministério da Saúde (Br). Envelhecimento e saúde da pessoa idosa. Brasília (DF): Ministério da Saúde; 2006.
14.Almeida STP. O perfil da caidora crônica no período do climatério assistida pelo Sistema Único de Saúde (SUS) [dissertação de mestrado]. Rio de Janeiro: Universidade Estácio de Sá; 2007.
15.Telles ACM. Prevalência, incidência, fatores preditivos e impacto das quedas entre as pessoas idosas no município de São Paulo: uma análise longitudinal [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 2008.
16.Aguiar JB, Paredes PFM, Gurgel LA. Análise da efetividade de um programa de hidroginástica sobre o equilíbrio, o risco de quedas e o IMC de mulheres idosas. RevBrasAtivFís Saúde. 2010; 15(2):115-9.
17.Souza CB, Abreu RNDC, Brit EM, Moreira TMM, Silva LMS, Vasconcelos SMM. O cuidado domiciliar de idosos acometidos por acidente vascular cerebral: cuidadores familiares. Rev Eletr Enferm. 2011; 13:395-404.
18.Lee JE, Stokic DS. Risk factors for falls during inpatient rehabilitation. Am J Phys Med Rehabil. 2008; 87:341-50.
19.Steadman MCSP, Donaldson N, Kalra MDA. Randomized controlled trial of an enhanced balance training program to improve mobility and reduce falls in elderly patients. J Am Geriat Soc. 2003; 51:847-52.
20.Berardinelli LMM, Santos I, Santos MLCS, Lima TCL, Missio AC, Berardinelli LM. Identificando vulnerabilidade para complicações cardiovasculares em idosos: uma estratégia para o cuidado. Rev enferm UERJ. 2011; 19:541-6.