RESEARCH ARTICLES
Assesment of the resilience level of adolescents with leprosy
Camila FernandesI; Beatriz Amorim BeltrãoII; Daniel Bruno Resende ChavesIII; Tânia Alteniza LeandroIV; Viviane Martins da SilvaV; Marcos Venícios de Oliveira LopesVI
INurse. Masters Student in Medical Microbiology at Universidade Federal do Ceará. Department of Medical Microbiology. Fortaleza, Ceará, Brazil. E-mail: camilabantim@hotmail.com.
IINurse. Masters Student in Nursing at Universidade Federal do Ceará. Department of Nursing. Fortaleza/Ceará, Brazil. E-mail: biaamorim@yahoo.com.br.
IIINurse. Masters in Nursing at Universidade Federal do Ceará. Department of Nursing. Fortaleza/Ceará, Brazil. E-mail: dbresende@yahoo.com.br.
IVStudent at Universidade Federal do Ceará. Department of Nursing. Fortaleza/Ceará, Brazil. E-mail: taniallt@yahoo.com.br.
VPhD in Nursing. Associate Professor II at Universidade Federal do Ceará. Departamento Department of Nursing. Fortaleza/Ceará, Brazil. E-mail: vivianemartinsdasilva@hotmail.com.
VIPhD in Nursing. Associate Professor I at Universidade Federal do Ceará. Department of Nursing. Fortaleza/Ceará, Brazil. E-mail: marcos@ufc.br.
ABSTRACT: The aim of the study was to evaluate the resilience level from 19 adolescents between 10 and 15 years old with leprosy, assisted in a reference center in dermatology in the city of Fortaleza. Exploratory and descriptive study with quantitative approach, happened in 2010, in which used one questionnaire and three scales. From total adolescents, 14 (73,7%) presented scores between 111 and 154 in the resilience scale from a maximum of 175. On the self-esteem scale, 16 (84,2%) of teenagers presented from 23 to 30 scores from a maximum of 40. Most of the values of the social support network scale ranged between 55 and 100 from a maximum of 100 scores. The adolescents showed direct relationship between the resilience scale scores and the scored of the social support network and self-esteem scale. The results emphasize the importance of new nursing studies that assess the resilience level of specific groups.
Keywords: Leprosy; resilience, psychological; adolescent; nursing.
INTRODUCTION
The nurse, as a professional working in primary care, plays an important role in the prevention of leprosy and monitoring of patients with this disease, especially among those individuals under the age of 15. Among his responsibilities, it is the nurse the one who assists in positive coping these individuals to the disease, strengthening protective factors, seeking the detection of risk factors by working with the family and support networks, and guide the patients on issues such as self-care to prevent disability and maintain a positive self-image.
The objective of this study was to evaluate the resilience of a group of teenagers, 10-15 years old, with leprosy.
LITERATURE REVIEW
Leprosy is a chronic infectious disease caused by Mycobacterium leprae bacillus gram-positive obligate intracellular with tropism for macrophages and Schwann cells, and that develops preferably in cold regions of the body1;. Despite its worldwide efforts to control and eradicate, the disease remains an important public health problem, especially in developing countries2.
In Brazil, the rate of detection of new leprosy cases has been increasing, especially in the age group between 10 and 15 years old. These cases have a direct relationship with foci of transmission assets and, since they are closely related to the endemicity of the region, have great relevance for the epidemiology of the disease3.
Leprosy is a disease historically seen with fear and prejudice by society4. Since the early days, people with leprosy were marginalized and their illness was regarded as divine punishment for their sins5. Unfortunately, this social condition still remains in many regions and interferes with the process of coping and / or resilience of patients.
Resilience is a dynamic process, which depends on the interaction of personal and intrapsychic human characteristics with aspects of the environment they live. It can be considered as an individual response towards risk, but it is not associated with the elimination of the stressor, but especially to a rehabilitation towards the patient6.
Currently, scholars seek strategies to positively affect on the process of resilience of individuals. With that, we try to make them able to face adverse situations that occur during life and to identify risk and protective factors that may influence this process7.
Risk factors represent individual and / or environmental obstacles that increase the vulnerability of the individual to develop physical, psychological and social disorders. Protective factors, in turn, relate to situations and or circumstances that influence the response of the individual, providing a positively overshoot to stressful events or situations8.
In general, adolescents are more vulnerable to biological stressors. Diseases such as leprosy and psychological stressors, arising from the stigma, represent a strong example of this situation. In this context, adolescents considered resilient are those able to actively seek help together with their associates and people they trust such as parents, teachers, students and certain groups9.
METHODOLOGY
This is an exploratory and descriptive study with a quantitative approach, performed on a secondary unit of dermatology health in Fortaleza, considered a benchmark in the diagnosis and treatment of leprosy. The study subjects were 19 adolescents between 10 and 15 years of age, with a diagnosis of leprosy, served in the unit in 2010. This group represented the total of teenagers registered and monitored in service in that year.
For data collection, the companion and adolescents were approached at the time waiting for appointments with the nurse unit. They were invited to address a nursing clinic available on the drive, to implement the instruments for data collection, which included a questionnaire and three rating scales. The questionnaire consisted of questions relevant to the epidemiology of leprosy in children under 15 years, and data related to risk and protective factors. Information relating to the questionnaire were obtained directly from the patient and their companion, while the data on the physical examination were obtained from medical records.
The evaluation of the degree of resilience based on the scale of Wagnild and Young. This scale ranges from 25 to 175 scores and consists of 25 items which follow a Likert scale, ranging from 1 to 710. The scale includes questions about the level of psychosocial adaptation in the face of life's adversities. It is divided into three dimensions: solving actions and values, with 14 items; independence and determination, with six items; confidence and ability to adapt to situations, with five items.
The level of self-esteem of these adolescents was evaluated based on the Rosenberg self-esteem scale. This instrument consists of 10 statements arranged in a Likert scale, for personal satisfaction, self-deprecation, perceived qualities, responsibility, pride in themselves, self-worth, respect and sense of failure.
The scale of social support network was applied to assess social support in the health/disease process experienced by adolescents. The scale consists of 19 items divided into five dimensions: material, emotional, affective, information, and positive social interaction.
The study was submitted to the Ethics and Research of the Reference Center for Sanitary Dermatology, in accordance with Resolution No. 196/96 on human research of the National Health Council which has approved registration with Opinion No. 12/1010. We sought to consent by signing the accompanying and adolescents Term of Consent.
The data relating to each of the assessments were organized in spreadsheets in Microsoft Excel ® 2007, and subsequently analyzed with the statistical package SPSS ® version 19.0. Statistical analysis determined whether the measures of central tendency and dispersion for numeric variables, and absolute frequencies and percentages for nominal variables. We used the Mann Whitney test to determine differences between media variables and Spearman test to check correlation. P values <0.05 were considered significant.
RESULTS AND DISCUSSION
The adolescents were aged between 10 and 14 years, predominantly, 8(42.1%), age 14 years, with a mean age of 12.68 years. Most were male, 11(57.9%), and were in elementary school 17(89.47%). Of these, 13(68.4%) reported living with former leprosy patients.
The fact that these teenagers are mostly males, corroborates the indicators shown in the official health surveillance in leprosy Ministry of Health 20083. In parallel, it is noteworthy that in 2007, 55.2% of leprosy cases in the country in teenagers under the age of 15 occurred in males. In the Northeast, the same indicator amounted to 52.1%. In a previous study, in Fortaleza, Ceará State, minors under 15 with leprosy were also predominantly male (58.8%)11. These data agree with the values obtained in the present study. The predominant age group of adolescents in this study also resembles previous studies, in which the detection rates of leprosy increased from the age of 14 years12.
As for previous vaccination by BCG, 18(94.7%) adolescents had received the 1st dose, and only 3(15.8%), 2nd dose. Among the respondents, 10(52.6%) were considered with multibacillary clinical form, according to the classification of the World Health Organization (WHO) based on number of injuries.
These findings confirm the results obtained in a previous study, in which 52.9% of those under 15 with leprosy, in Fortaleza, were classified as multibacillary. It is noteworthy that, according to the same author, in 2001 this statistic was reversed. The paucibacillary were more frequent (55.3%), reaching peak of 67.1% in 2006 and reversing the prevalence in 2007, as mentioned11.
The teens were also evaluated for the presence or absence of influential factors (protective or risk) of resilience. The factor family income ranged from one to four minimum wages, and 12(63.2%) adolescents reported income from a salary. Regarding the use of drugs in the family, 12(63.2%) subjects reported having no family who used licit or illicit drugs. Individuals, mostly schoolchildren showed no problems, as mentioned 17(89.5%) adolescents. We could see that 15(78.9%) subjects had some kind of illness in the family, such as leprosy, diabetes, hypertension, heart disease, malignancy and depression. As for the loss factor in the family, 14(73.7%) adolescents reported not having experienced this situation recently. As for religious habits, 11(57.9%) adolescents reported going to church, even occasionally. All respondents reported having friends, 12(63.2%) reported having some kind of religion, and having divorced parents.
Some influencing factors of resilience are also considered risk or protective factors associated with leprosy. Regarding risk factors, studies show that levels of endemic disease, unfavorable socioeconomic conditions, poor living conditions and health and the high number of people living in the same environment, influence the risk of becoming sick13. In this context, the intimate and prolonged contact with people affected by leprosy is a risk factor for the disease, very often at home14. Besides household contact, most incident cases could be related to a previous case of leprosy, such as the tuberculosis15. An earlier study enabled us to verify that the family income of adolescents with leprosy is low, being another important risk factor. In this study it was observed that this disease is most present in class socially weaker of society16. Still, according to the same study, it was observed that all teenagers had some degree of schooling, indicating that appropriate interventions should be implemented according to the education level of these individuals16. These findings corroborate the present study, because 13(68.4%) adolescents reported living former leprosy patients, 15(78.9%) had some type of illness in the family, 12(63.2%) reported an income salary and 17(89.47%) reported no problems in school and were in elementary school.
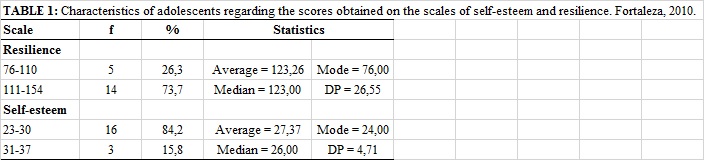
The scores obtained with the application of the resilience scale ranged 76-154. On this scale, 14(73.7%) adolescents had scores between 111 and 154 out of 175. The average score was 123.26 and a standard deviation of 26.55, as shown in Table 1. These findings confirm with the results of other authors, in which much of leprosy patients showed high scores on the resilience scale17.
On the scale of self-esteem, 16(84.2%) youth had 23-30 scores a maximum total of 40. Scores ranged 23-37, with an average of 27.37 and a standard deviation of 4.11, according to Table 1. These moderate scores (23-30 points) opposed to the idea suggested in studies conducted in the State of São Paulo, which revealed that leprosy has long been stigmatized by society and, in most cases, change the self-image of the individual, causing them fear of social rejection and decreased self-esteem18.
After analyzing the differences in median scale scores self-esteem among adolescents classified as paucibacillary and multibacillary, it was observed that the paucibacillary had, in this study, higher values on the scale of self-esteem than the multibacillary. Studies show that multibacillary patients are more susceptible to physical changes, for presenting high bacillary load. This may influence the self-esteem of adolescents16.
On the scale of self-esteem, girls had higher scores than boys, in contrast to the results obtained in another study. Findings in the literature report that, compared to men, women with leprosy have greater change in self-esteem, caused by changes in self-image resulting from the illness18. Such divergences between literature and the findings of this study can be explained by the difference in the number of injuries in relation to gender. In this work, we observed that, compared to boys, girls showed skin changes with less intensity. This is evidenced by the fact that 5(55.5%) girls had from one to five lesions, whereas only 4(30%) of the boys had less than five lesions.
Each dimension of the scale of social support network was analyzed separately, and each dimension could reach a maximum value of 100 scores. Most adolescents, 15(78.9%), got score between 76 and 100 in the material dimension of the scale. The mean score was 82.89 and the standard deviation of 16.35. The affective, 14(73.7%) adolescents had scores between 71 and 100, with an average of 84.47 and a standard deviation of 19.94. The emotional dimension, 10(52.6%) youth had scores between 71 and 100, with an average of 74.21 and a standard deviation of 20.01. In the dimension of information, 10(52.6%) respondents had scores between 55 and 80, with a mean of 77.11 and standard deviation 15.66. While, in the dimension of positive social interaction, 16(84.2%) subjects had scores between 61 and 100, with mean values of 78.95 and a standard deviation of 21.76.
As noted, most of the adolescents had higher scores in the dimensions material, affective, emotional, and positive social interaction scale social support network. The size information was associated with lower scores. This is justified by the fact that the family income of the majority of the subjects are of a minimum wage, which complicates the process of education and information use.
Also in relation to the scores of the scales, it should be noted that there were no statistically significant differences in the median scores for classification of paucibacillary and multibacillary as well as between male and female.
Teens with multibacillary clinical form proved more resilient than paucibacillary, suggesting that the number of injuries seems no to be a risk factor in the population studied, or that this factor alone is not a predictor of resilience. Paradoxically, if you think that the level of self-esteem of paucibacillary was higher than that of multibacillary and that high self-esteem is a protective factor of resilience, it was expected that the paucibacillary also be more resilient than the multibacillary. This difference reinforces the context of adversity necessary for resilience is defined by the combination of the quantity, nature and intensity of risk factors6.
Regarding gender, boys were more resilient than girls, this contrasts with other studies, whose healthy adolescent females were more resilient than males6. The physiological and psychological differences between adolescent males and females can justify the fact that girls are less resilient in this study. In adolescent girls, the bodily and psychological changes cause most impact.
When evaluating the effects of the disease in men and women, another study found that both are equally affected by the disease. Moreover, the leprosy patients, especially women, are concerned about the appearance, self-esteem, emotional state, sexuality and social interaction, whereas men are more concerned with the impossibility or force reduction19. It is clear, then, that women were more prejudiced against themselves than men.
The influence factor separated parents showed a statistically significant difference in averages (p = 0.047). Teens with divorced parents had lower values on the resilience scale, being a negative factor for the degree of resilience, as exposed in Table 2. This fact was not verified previously by other authors among adolescents with leprosy. On the other hand, studies on resilience in adolescents, independent of the type of disease, showed statistical significance with the experience of parental separation6.
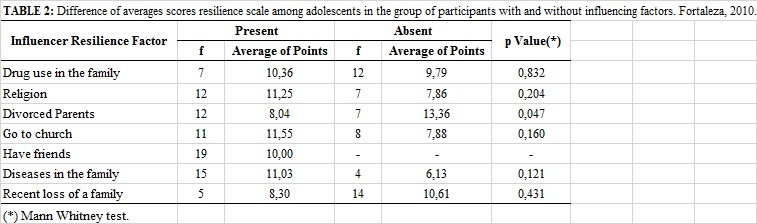 .
.
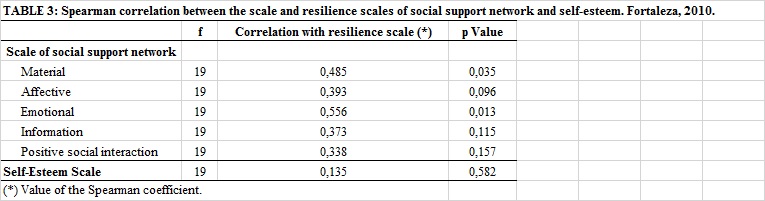
The correlation of material and emotional dimensions of the scale of social support network with resilience scale showed statistically significance, suggesting that the relation between them is directly proportional (p = 0.035 and p = 0.013, respectively), according to Table 3. Therefore, it was observed that adolescents with higher material and emotional support have higher scores on the resilience scale. Although other dimensions of scale have not presented statistically significant values in young people assessed the direct relationship with resilience remained in all dimensions of the scale. This is similar to results from other studies in which the scale of social network had a direct relationship with the resilience scale, indicating the importance of social support for the formation of the resilience6.
The scale of self-esteem also maintained a direct relationship with the resilience scale, although no statistical significance. This effect was also shown in a previous study in which it was found that, as the level of self-esteem decay can be observed decrease in the levels of resilience6.
CONCLUSION
Most adolescents were male, with the predominant age of 14. These were classified, in the majority, the clinical multibacillary form and attending elementary school. As for the risk or protective factors (resilience influencers), most had family income of a minimum wage, family diseases, religion, divorced parents, and friends. In addition to the family income, there are factors affecting disease such as: interaction with previous leprosy patients, some kind of illness in the family, and schooling.
As for the scores obtained on the scale of resilience, values generally ranged from moderate to strong, noting a difference between the genders, in which boys were more resilient than girls. While, on the scale of self-esteem, young people had scores of moderate to strong, getting girls score higher than boys. On the scale of social support network, girls have higher scores on the dimensions material, affective and positive social interaction, differing from the boys, who scored higher for emotional and information.
Some limitations were encountered in this study. One was the small sample size, which prevents generalization of findings. The other refers to the facts of the scores of the scales used (self-esteem, resilience and social support) do not submit cutoff pre-defined in the literature. Still, there is scant literature on resilience of adolescents with leprosy. Therefore, this study emphasizes the importance of new nursing studies that assess the degree of resilience of specific groups. Such knowledge may encourage nurses to promote health, shifting the emphasis on the negative potential of the disease to the family and individual.
REFERENCES
1. Ministério da Saúde (Br). Guia de Vigilância Epidemiológica. Brasília (DF): Ministério da saúde; 2010.
2. Secretaria Municipal de Saúde (Fortaleza). Informe epidemiológico: hanseníase. Fortaleza (CE): Secretaria Municipal de Sáude; 2008.
3. Ministério da Saúde (Br). Vigilância em saúde: situação epidemiológica da hanseníase no Brasil. Brasília (DF): Editora MS; 2008.
4. Bittencourt LP, Carmo AC, Leão AMM, Clos AC. Estigma: percepções sociais reveladas por pessoas acometidas por hanseníase. Rev enferm UERJ. 2010; 18: 185-90.
5. Boti NCL, Aquino KA. A via sacra da hanseníase de veganin. Rer Bras Enferm. 2008; 61: 676-81.
6. Pesce RP, Assis SG, Santos N, Oliveira RVC. Risco e proteção: em busca de um equilíbrio promotor de resiliência. Psicologia: Teoria e Pesquisa. 2004; 20: 135-43.
7. Pinheiro DPN. A resiliência em discussão. Psicologia em estudo. 2004; 9: 67-75.
8. Carvalho FT, Morais NA, Koller SH, Piccinini CA. Fatores de proteção relacionados à promoção de resiliência em pessoas que vivem com HIV/AIDS. Cad Saúde Pública. 2007; 23: 2023-33.
9. Silva MRS, Lunardi VL, Filho WDL, Tavares KO. Resiliência e promoção da saúde. Texto contexto - enferm. 2005; 14: 95-102.
10. Pesce RP, Assis SG, Avanci JQ, Santos NC, Malaquias JV, Carvalhaes R. Adaptação transcultural, confiabilidade e validade da escala de resiliência. Cad Saúde Pública. 2005; 21: 436-48.
11. Alencar CHM, Barbosa JC, Ramos NA, Alencar MJF, Pontes RJS, Castro CGJ, Heukelbach J. Hanseníase no município de Fortaleza, CE, Brasil: aspectos epidemiológicos e operacionais em menores de 15 anos. Rev Bras Enferm. 2008; 61: 694-700.
12. Lanza FM, Cortez DN, Gontijo TL, Rodrigues JSJ. Perfil epidemiológico da hanseníase no município de Divinópolis, Minas Gerais. Rev Enferm UFSM. 2012; 2: 365-74.
13. Ministério da Saúde (Br). Guia para controle da hanseníase. Brasília (DF): Ministério da Saúde; 2002.
14. Ministério da Saúde (Br). Vigilância em Saúde: Dengue, Esquistossomose, Hanseníase, Malária, Tracoma e Tuberculose. 2ª ed. rev. Brasília (DF): Ministério da Saúde; 2008.
15. Sanches LAT, Pitter E, Sanches HF, Monteiro MC. Detecção de casos novos de hanseníase no município de Prudentópolis, PR: uma análise de 1998 a 2005. Revista da Sociedade Brasileira de Medicina Tropical. 2007; 40: 541-5.
16. Ponte KMA, Ximenes Neto FRG. Hanseníase: a realidade do ser adolescente. Rev Bras Enferm. 2005; 58: 296-301.
17. Godas ML. Resiliência e comportamento de autocuidado em pacientes atingidos pela hanseníase: relação positiva?. Programa de aprimoramento profissional. Bauru (SP): Secretaria do Estado da Saúde; 2010.
18. Palmeira IP, Queiroz ABA, Ferreira MA. Quando o preconceito marca mais que a doença. Tempus - Actas de Saúde Coletiva. 2012; 6: 187-99.
19. Santos AK, Ribeiro APG, Monteiro S. Hanseníase e práticas da comunicação: estudo de recepção de materiais educativos em um serviço de saúde no Rio de Janeiro. Interface – Comunic, Saude, Educ. 2012; 16: 205-18.